Tricyclic Antidepressants
Tricyclic antidepressants (TCAs) are a drug class that was first released to the market in 1959 as a pharmacotherapy for major depressive disorder (MDD). Today, TCAs are Food and Drug Administration (FDA) approved to treat a variety of illnesses, depending on the formulation. TCAs that have FDA approval to treat MDD include amitriptyline, amoxapine, doxepin, desipramine, nortriptyline, protriptyline, imipramine, and trimipramine.[1][2][3][4] Clomipramine is FDA approved for obsessive-compulsive disorder (OCD) in ages ten and older.[5]
In terms of treating major depressive disorder, TCAs display equivocal efficacy with Selective Serotonin Reuptake Inhibitors (SSRIs), but TCAs cause more significant adverse effects due to their anticholinergic activity and a lower threshold for overdose.[6][7] For these reasons, TCAs typically are not used as first-line treatment of MDD.[8] The off-label (non-FDA) uses of TCAs include migraine prophylaxis, OCD, insomnia, anxiety, and chronic pain, especially neuropathic pain conditions such as myofascial pain, diabetic neuropathy, and postherpetic neuralgia.[9][10][11][12][13][14][15] Specifically, for migraine prophylaxis, doxepin and amitriptyline are most commonly used.[16][17] TCAs are also the second-line treatment for fibromyalgia after the failure of preferred treatments, such as pregabalin, duloxetine, and milnacipran.[18][19] Nocturnal enuresis of children is also treatable with TCAs after the failure of first-line therapy desmopressin.[20]
Conditions Treated
Tricyclic antidepressants are used primarily to treat mood disorders but also have their place in the treatment of anxiety disorders, personality disorders, and neurological disorders.2 They are often used when other drugs are unable to provide relief.
Mood disorders often treated with TCAs include:
- Bipolar disorder
- Dysthymia (persistent mild depression)
- Major depressive disorder (MDD)
Anxiety disorders sometimes treated with TCAs include:
- Body dysmorphic disorder (BDD), including eating disorders such as anorexia nervosa and bulimia nervosa
- Generalized anxiety disorder (GAD)
- Obsessive-compulsive disorder (OCD)
- Panic disorder (PD)
- Post-traumatic stress disorder (PTSD)
Neurological disorders sometimes treated with tricyclic TCAs include:
- Attention-deficit hyperactivity disorder (ADHD)
- Chronic pain
- Fibromyalgia
- Parkinson’s disease
- Migraine
- Neuropathic pain
Mechanism of Action
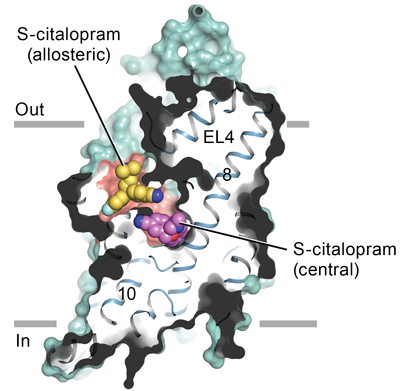
Tricyclic antidepressants act on approximately five different neurotransmitter pathways to achieve their effects. They block the reuptake of serotonin and norepinephrine in presynaptic terminals, which leads to increased concentration of these neurotransmitters in the synaptic cleft. The increased concentrations of norepinephrine and serotonin in the synapse likely contributes to its anti-depressive effect. Additionally, they act as competitive antagonists on post-synaptic alpha cholinergic (alpha1 and alpha2), muscarinic, and histaminergic receptors (H1).[21][22] Its structure greatly influences the affinity of the TCA for each of these receptors.
The chemical structure of a TCA consists of a three-ringed structure with an attached secondary or tertiary amine. Secondary amines include desipramine, nortriptyline, and protriptyline, while tertiary amines consist of amitryptiline, clomipramine, doxepin, imipramine, and trimipramine. Tertiary amines tend to have greater blockage of serotonin reuptake, while secondary amines have greater blockage of norepinephrine uptake.[23] The combination of different amine structures and variations in chemical composition contribute to the multitude of adverse effects seen with TCA usage as these factors affect TCA-receptor affinity and binding.[24]
Administration
TCAs are available in the form of oral tablets, capsules, and solutions. Although intravenous (IV) use of some TCAs, such as clomipramine, has taken place in clinical trials, IV is not a routine route of administration for the administration of TCAs.[25] Topical creams and transdermal patches have been studied for the use of some TCAs, like imipramine and doxepin, as well. However, oral administration (PO) remains the usual route of administration for TCAs.[26] The exact dosages for each of the different TCA tablets vary, however, because TCAs have a high risk of adverse effects, initial dosing is low and is gradually increased based on the level of response.[27] If patients are unresponsive at a low dose, then they may respond at higher doses, especially since TCAs have shown increased efficacy at higher dosages when compared with high dose SSRIs.[27] Blood monitoring of TCA concentrations is available; however, there is mixed evidence on its effect on treatment outcomes.[7] In general, patients are given an oral dose of a TCA once a day due to the long half-life and sedative effects of the drug class.[24]
Approved Medications
With tricyclic antidepressants, like other antidepressants, it will usually take between six to eight weeks before you feel any substantial improvement in your depression symptoms.3 Some of the more commonly prescribed TCAs include:
- Anafranil (clomipramine)
- Ascendin (amoxapine)
- Elavil (amitriptyline)
- Norpramin (desipramine)
- Pamelor (nortriptyline)
- Sinequan (doxepin)
- Surmontil (trimipramine)
- Tofranil (imipramine)
- Vivactil (protriptyline)
Common Side Effects
While different TCAs have slightly different mechanisms of action, they share similar side effects. Many of these are associated with the effect the drugs have on the smooth muscles of the internal organs. Common side effects include:
- Anxiety
- Blurred vision
- Constipation
- Dizziness
- Drowsiness
- Increased appetite
- Muscle twitches
- Nausea and vomiting
- Rapid or irregular heart rate
- Sexual dysfunction
- Sweating
- Weakness
- Weight gain
These side effects may be reduced if treatment is started with lower dosages and then gradually increased. While not strictly addictive per se, the long-term use of TCAs may lead to drug dependence.
TCAs are also a significant cause of fatal drug overdoses in the United States.4 Initial symptoms may include dry mouth, blurred vision, urinary retention, constipation, dizziness, vomiting, and hallucinations. If left untreated, an overdose may result in delirium, seizures, coma, cardiac arrest, and death.
Adverse Effects
TCAs have varying degrees of receptor affinities, leading to several adverse effects. The most common adverse effects include constipation, dizziness, and xerostomia[28]. Due to its blockade of cholinergic receptors, it can lead to blurred vision, constipation, xerostomia, confusion, urinary retention, and tachycardia.[29] Due to the blockade of alpha-1 adrenergic receptors, it can cause orthostatic hypotension and dizziness.[28][29] TCA-induced histamine blockade (H1) may lead to sedation, increased appetite, weight gain, and confusion.[30][28]
TCAs may also cause cardiovascular complications, including arrhythmias, such as QTc prolongation, ventricular fibrillation, and sudden cardiac death in patients with preexisting ischemic heart disease.[31] Therefore, the examination of a patient’s cardiac health is important before TCA prescription. there is evidence of TCAs increasing the risk of seizures in those with epilepsy, and use requires caution in this population.[32] TCAs may cause mild liver enzyme elevation; however, acute hepatitis rarely has an association with the use of tricyclic antidepressants.[30][33]
TCA use has shown to lead to an increased risk of suicidal ideation and behavior in individuals age 24 or less. Therefore, individuals started on TCAs that are age 24 or less should be followed closely to assess for thoughts and behaviors related to suicide.[33]
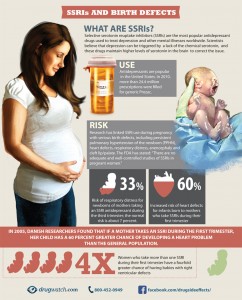
The use of TCAs during pregnancy has correlated with congenital eye, ear, face, and neck defects.[34] Specifically, clomipramine has associations with more severe neonatal symptoms such as cardiac defects.[35] Therefore, TCAs are not generally considered safe to use during pregnancy. With regards to breastfeeding, all TCAs, except for doxepin, have not been associated with adverse effects from breastfeeding and therefore are regarded as safe.[36] Nortriptyline appears to be the safest for use during breastfeeding due to its non-sedating profile.[35]
Contraindications
Tricyclic antidepressants are contraindicated in several populations and with the concomitant use of various medications. TCAs should not be prescribed if there is a family history of QTc interval prolongation or sudden cardiac death. Hypersensitivity reactions to a TCA drug are considered an absolute contraindication. However, patients with a hypersensitivity reaction to a particular TCA drug may be prescribed a different member of the class with caution. TCAs should not be used concomitantly with monoamine oxidase inhibitors (MAOI), e.g., phenelzine, due to the risk of developing serotonin syndrome.[37] Also, patients must have discontinued MAOI for at least 14 days before starting a TCA medication. Combining TCAs with SSRIs is not advised as a combination of these agents has been shown to increase plasma concentrations of TCAs and risk of serotonin syndrome.[38][39]
TCA use requires caution in individuals with angle-closure glaucoma as its anticholinergic effects may increase the risk of an acute ocular crisis.[40] Additionally, TCAs should be used with caution in patients with a history of seizures, as TCAs may lower the seizure threshold, and in patients with urinary retention, as its anticholinergic properties may worsen this symptom.[29][32] Clinicians should generally avoid TCAs in patients with coronary artery disease (CAD). However, CAD is not an absolute contraindication.[41] Because cytochrome P450 enzymes metabolize TCAs in the liver, caution is necessary when prescribing TCAs to patients with hepatic injury. Specifically, among the TCAs, clomipramine has been shown to have the highest rate of drug-induced liver injury, and so clomipramine is not preferred in patients with non-optimal liver function.[42]
Monitoring
Overall, the therapeutic index of TCAs is narrow, and the therapeutic range for each specific TCA is dependent on the drug prescribed. Because of the narrow therapeutic index of TCAs, patients should be monitored closely for symptoms of toxicity, i.e., QRS-widening on electrocardiogram (ECG), tremors, confusion, muscle rigidity, and coma.[23]
All patients starting a TCA need screening for pre-existing cardiac conditions, including prolonged QTc intervals, heart disease, and a family history of arrhythmias. Patients who test positive for pre-existing heart conditions may need additional evaluation by a cardiologist before initiating treatment. Additionally, these patients require regular monitoring for the presence of new cardiac symptoms. Patients with low potassium blood concentrations should have periodical monitoring to reduce the risk of arrhythmias.[31] In patients over the age of 50, obtaining an ECG is recommended.
All patients starting a TCA or presently taking a TCA should be monitored for worsening depressive symptoms or new-onset suicidal thoughts or behaviors. It may be helpful to monitor the blood concentrations of TCAs in non-adherent patients, have decreased tolerability, or little response to the drug. However, there is mixed evidence on the effectiveness of blood concentration monitoring on clinical outcomes.[7]
Toxicity
Tricyclic antidepressants (TCAs) generally have a narrow therapeutic index and, therefore, are prone to induce toxicity if intentional overdose occurs. They have demonstrated higher rates of death per one million prescriptions when compared to other antidepressants due to higher rates of suicide by deliberate overdose.[43] Older TCAs, such as desipramine, nortriptyline, and trimipramine, have been shown to induce toxicity at lower doses than newer TCAs, such as amitriptyline.
Symptoms of overdose include ECG abnormalities such as QTc prolongation and widened QRS complex, hypotension, seizures, tremors, coma, xerostomia, urinary retention, and respiratory depression.[44] Death from TCAs most commonly occurs due to hypotension or arrhythmias.[45] Treatment of TCA overdose requires the stabilization of the patient and efficiently addressing the acute complications. Activated charcoal may be given for TCA overdose to prevent the absorption of the drug, but activated charcoal administration must be within 2 hours of TCA ingestion.[46] Patients with a prolonged QRS interval should receive sodium bicarbonate to increase the pH of the serum and reduce the concentration of active free TCA medication.[47] In cases of TCA-induced cardiotoxicity that is non-responsive to sodium bicarbonate, lidocaine may be an option as a reversal agent.[45] Patients with TCA-induced seizures should receive benzodiazepines for treatment.[48] Patients that develop hypotension need IV crystalloids, and patients with signs of respiratory compromise should receive respiratory support. Patients with hypotension that is non-responsive to crystalloids should have a trial of norepinephrine.[49]
TCAs should not be used concomitantly with monoamine oxidase inhibitors (MAOI) due to the risk of developing serotonin syndrome.[37] Serotonin syndrome presents with dilated pupils, hyperreflexia, myoclonus, diarrhea, tremors, and confusion. Treatment for serotonin syndrome includes cooling, discontinuation of serotonergic drugs, and cyproheptadine.
Enhancing Healthcare Team Outcomes
Tricyclic antidepressants (TCAs) are a class of antidepressants that are commonly prescribed for off-label use today. Although TCAs may be prescribed for MDD, they are seldom prescribed as a first-line treatment due to their unfavorable adverse effect profile, i.e., anticholinergic, antihistamine, and antiadrenergic effects, and because there are many safer alternatives available, such as SSRIs. However, TCAs may be prescribed for MDD if more conservative antidepressant pharmacotherapy has failed. Regardless of the indications for TCAs, patients who require treatment with TCAs need the involvement of an interprofessional team to help maintain patient safety.
Coordination between a patient’s primary care physician, psychiatrist, and possibly cardiologist if cardiac function abnormalities are present is essential for maintaining patient stability and preventing adverse outcomes. Patient monitoring for suicidal intent is necessary to avoid toxicity and overdose.[50] Additionally, communication between a cardiologist and a prescribing physician is essential to prevent cardiotoxic outcomes in patients with predisposing risk-factors for cardiac dysfunction.[31]
Pharmacists should have involvement in the care of patients prescribed TCAs. Pharmacists can confirm the appropriate dosage and can recognize critical drug-drug interactions. Also, TCAs primarily undergo metabolism in the liver, so pharmacists can reduce the risk of interaction with other drugs by identifying the concomitant use of drugs that influence hepatic metabolism.[51] Nurses can assist in assessing patient adherence and monitoring patients for adverse effects. Open and frequent communication between all members of the interprofessional healthcare team should occur to ensure the best possible patient care outcomes. [Level 5]
Continuing Education / Review Questions
- Access free multiple choice questions on this topic.
- Earn continuing education credits (CME/CE) on this topic.
- Comment on this article.
- 1.
- Dopheide JA. Recognizing and treating depression in children and adolescents. Am J Health Syst Pharm. 2006 Feb 01;63(3):233-43. [PubMed]
- 2.
- Stokes PRA, Jokinen T, Amawi S, Qureshi M, Husain MI, Yatham LN, Strang J, Young AH. Pharmacological Treatment of Mood Disorders and Comorbid Addictions: A Systematic Review and Meta-Analysis: Traitement Pharmacologique des Troubles de L’humeur et des Dépendances Comorbides: Une Revue Systématique et une Méta-Analyse. Can J Psychiatry. 2020 Nov;65(11):749-769. [PMC free article] [PubMed]
- 3.
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. National Institute of Diabetes and Digestive and Kidney Diseases; Bethesda (MD): Apr 27, 2018. Antidepressant Agents. [PubMed]
- 4.
- Boafo A, Greenham S, Sullivan M, Bazaid K, Suntharalingam S, Silbernagel L, Magner K, Robillard R. Medications for sleep disturbance in children and adolescents with depression: a survey of Canadian child and adolescent psychiatrists. Child Adolesc Psychiatry Ment Health. 2020;14:10. [PMC free article] [PubMed]
- 5.
- Del Casale A, Sorice S, Padovano A, Simmaco M, Ferracuti S, Lamis DA, Rapinesi C, Sani G, Girardi P, Kotzalidis GD, Pompili M. Psychopharmacological Treatment of Obsessive-Compulsive Disorder (OCD). Curr Neuropharmacol. 2019;17(8):710-736. [PMC free article] [PubMed]
- 6.
- Anderson IM. Selective serotonin reuptake inhibitors versus tricyclic antidepressants: a meta-analysis of efficacy and tolerability. J Affect Disord. 2000 Apr;58(1):19-36. [PubMed]
- 7.
- Thorstrand C. Clinical features in poisonings by tricyclic antidepressants with special reference to the ECG. Acta Med Scand. 1976;199(5):337-44. [PubMed]
- 8.
- von Wolff A, Hölzel LP, Westphal A, Härter M, Kriston L. Selective serotonin reuptake inhibitors and tricyclic antidepressants in the acute treatment of chronic depression and dysthymia: a systematic review and meta-analysis. J Affect Disord. 2013 Jan 10;144(1-2):7-15. [PubMed]
- 9.
- Xu XM, Liu Y, Dong MX, Zou DZ, Wei YD. Tricyclic antidepressants for preventing migraine in adults. Medicine (Baltimore). 2017 Jun;96(22):e6989. [PMC free article] [PubMed]
- 10.
- Clomipramine in the treatment of patients with obsessive-compulsive disorder. The Clomipramine Collaborative Study Group. Arch Gen Psychiatry. 1991 Aug;48(8):730-8. [PubMed]
- 11.
- Max MB, Lynch SA, Muir J, Shoaf SE, Smoller B, Dubner R. Effects of desipramine, amitriptyline, and fluoxetine on pain in diabetic neuropathy. N Engl J Med. 1992 May 07;326(19):1250-6. [PubMed]
- 12.
- Hayashida KI, Obata H. Strategies to Treat Chronic Pain and Strengthen Impaired Descending Noradrenergic Inhibitory System. Int J Mol Sci. 2019 Feb 14;20(4) [PMC free article] [PubMed]
- 13.
- Pilowsky I, Hallett EC, Bassett DL, Thomas PG, Penhall RK. A controlled study of amitriptyline in the treatment of chronic pain. Pain. 1982 Oct;14(2):169-79. [PubMed]
- 14.
- Pal US, Kumar L, Mehta G, Singh N, Singh G, Singh M, Yadav HK. Trends in management of myofacial pain. Natl J Maxillofac Surg. 2014 Jul-Dec;5(2):109-16. [PMC free article] [PubMed]
- 15.
- Berger A, Dukes E, Edelsberg J, Stacey B, Oster G. Use of tricyclic antidepressants in older patients with diabetic peripheral neuropathy. Clin J Pain. 2007 Mar-Apr;23(3):251-8. [PubMed]
- 16.
- Radley DC, Finkelstein SN, Stafford RS. Off-label prescribing among office-based physicians. Arch Intern Med. 2006 May 08;166(9):1021-6. [PubMed]
- 17.
- Punay NC, Couch JR. Antidepressants in the treatment of migraine headache. Curr Pain Headache Rep. 2003 Feb;7(1):51-4. [PubMed]
- 18.
- Calandre EP, Rico-Villademoros F, Slim M. An update on pharmacotherapy for the treatment of fibromyalgia. Expert Opin Pharmacother. 2015 Jun;16(9):1347-68. [PubMed]
- 19.
- Häuser W, Bernardy K, Uçeyler N, Sommer C. Treatment of fibromyalgia syndrome with antidepressants: a meta-analysis. JAMA. 2009 Jan 14;301(2):198-209. [PubMed]
- 20.
- Gepertz S, Nevéus T. Imipramine for therapy resistant enuresis: a retrospective evaluation. J Urol. 2004 Jun;171(6 Pt 2):2607-10; discussion 2609-10. [PubMed]
- 21.
- Hillhouse TM, Porter JH. A brief history of the development of antidepressant drugs: from monoamines to glutamate. Exp Clin Psychopharmacol. 2015 Feb;23(1):1-21. [PMC free article] [PubMed]
- 22.
- Richelson E. Antimuscarinic and other receptor-blocking properties of antidepressants. Mayo Clin Proc. 1983 Jan;58(1):40-6. [PubMed]
- 23.
- Gillman PK. Tricyclic antidepressant pharmacology and therapeutic drug interactions updated. Br J Pharmacol. 2007 Jul;151(6):737-48. [PMC free article] [PubMed]
- 24.
- Hiemke C, Baumann P, Bergemann N, Conca A, Dietmaier O, Egberts K, Fric M, Gerlach M, Greiner C, Gründer G, Haen E, Havemann-Reinecke U, Jaquenoud Sirot E, Kirchherr H, Laux G, Lutz UC, Messer T, Müller MJ, Pfuhlmann B, Rambeck B, Riederer P, Schoppek B, Stingl J, Uhr M, Ulrich S, Waschgler R, Zernig G. AGNP Consensus Guidelines for Therapeutic Drug Monitoring in Psychiatry: Update 2011. Pharmacopsychiatry. 2011 Sep;44(6):195-235. [PubMed]
- 25.
- Pallanti S, Hollander E, Bienstock C, Koran L, Leckman J, Marazziti D, Pato M, Stein D, Zohar J., International Treatment Refractory OCD Consortium. Treatment non-response in OCD: methodological issues and operational definitions. Int J Neuropsychopharmacol. 2002 Jun;5(2):181-91. [PubMed]
- 26.
- Sandig AG, Campmany AC, Campos FF, Villena MJ, Naveros BC. Transdermal delivery of imipramine and doxepin from newly oil-in-water nanoemulsions for an analgesic and anti-allodynic activity: development, characterization and in vivo evaluation. Colloids Surf B Biointerfaces. 2013 Mar 01;103:558-65. [PubMed]
- 27.
- Adli M, Baethge C, Heinz A, Langlitz N, Bauer M. Is dose escalation of antidepressants a rational strategy after a medium-dose treatment has failed? A systematic review. Eur Arch Psychiatry Clin Neurosci. 2005 Dec;255(6):387-400. [PubMed]
- 28.
- Trindade E, Menon D, Topfer LA, Coloma C. Adverse effects associated with selective serotonin reuptake inhibitors and tricyclic antidepressants: a meta-analysis. CMAJ. 1998 Nov 17;159(10):1245-52. [PMC free article] [PubMed]
- 29.
- Güloglu C, Orak M, Ustündag M, Altunci YA. Analysis of amitriptyline overdose in emergency medicine. Emerg Med J. 2011 Apr;28(4):296-9. [PubMed]
- 30.
- David DJ, Gourion D. [Antidepressant and tolerance: Determinants and management of major side effects]. Encephale. 2016 Dec;42(6):553-561. [PubMed]
- 31.
- Fanoe S, Kristensen D, Fink-Jensen A, Jensen HK, Toft E, Nielsen J, Videbech P, Pehrson S, Bundgaard H. Risk of arrhythmia induced by psychotropic medications: a proposal for clinical management. Eur Heart J. 2014 May 21;35(20):1306-15. [PubMed]
- 32.
- Johannessen Landmark C, Henning O, Johannessen SI. Proconvulsant effects of antidepressants – What is the current evidence? Epilepsy Behav. 2016 Aug;61:287-291. [PubMed]
- 33.
- Drug interactions with selective serotonin reuptake inhibitors, especially with other psychotropics. Prescrire Int. 2001 Feb;10(51):25-31. [PubMed]
- 34.
- Bérard A, Zhao JP, Sheehy O. Antidepressant use during pregnancy and the risk of major congenital malformations in a cohort of depressed pregnant women: an updated analysis of the Quebec Pregnancy Cohort. BMJ Open. 2017 Jan 12;7(1):e013372. [PMC free article] [PubMed]
- 35.
- Gentile S. Tricyclic antidepressants in pregnancy and puerperium. Expert Opin Drug Saf. 2014 Feb;13(2):207-25. [PubMed]
- 36.
- Lanza di Scalea T, Wisner KL. Antidepressant medication use during breastfeeding. Clin Obstet Gynecol. 2009 Sep;52(3):483-97. [PMC free article] [PubMed]
- 37.
- Schipper P, Vanmolkot L, Peeters FP. [Combining a classic monoamine oxidase inhibitor with a tricyclic antidepressant in therapy-resistant depression: a case report and literature review]. Tijdschr Psychiatr. 2016;58(12):886-890. [PubMed]
- 38.
- Dunner DL. Combining antidepressants. Shanghai Arch Psychiatry. 2014 Dec;26(6):363-4. [PMC free article] [PubMed]
- 39.
- Taylor D. Selective serotonin reuptake inhibitors and tricyclic antidepressants in combination. Interactions and therapeutic uses. Br J Psychiatry. 1995 Nov;167(5):575-80. [PubMed]
- 40.
- Lieberman E, Stoudemire A. Use of tricyclic antidepressants in patients with glaucoma. Assessment and appropriate precautions. Psychosomatics. 1987 Mar;28(3):145-8. [PubMed]
- 41.
- Cohen HW, Gibson G, Alderman MH. Excess risk of myocardial infarction in patients treated with antidepressant medications: association with use of tricyclic agents. Am J Med. 2000 Jan;108(1):2-8. [PubMed]
- 42.
- Friedrich ME, Akimova E, Huf W, Konstantinidis A, Papageorgiou K, Winkler D, Toto S, Greil W, Grohmann R, Kasper S. Drug-Induced Liver Injury during Antidepressant Treatment: Results of AMSP, a Drug Surveillance Program. Int J Neuropsychopharmacol. 2016 Apr;19(4) [PMC free article] [PubMed]
- 43.
- Henry JA. A fatal toxicity index for antidepressant poisoning. Acta Psychiatr Scand Suppl. 1989;354:37-45. [PubMed]
- 44.
- Starkey IR, Lawson AA. Poisoning with tricyclic and related antidepressants–a ten-year review. Q J Med. 1980 Winter;49(193):33-49. [PubMed]
- 45.
- Pentel PR, Benowitz NL. Tricyclic antidepressant poisoning. Management of arrhythmias. Med Toxicol. 1986 Mar-Apr;1(2):101-21. [PubMed]
- 46.
- Hultén BA, Adams R, Askenasi R, Dallos V, Dawling S, Heath A, Volans G. Activated charcoal in tricyclic antidepressant poisoning. Hum Toxicol. 1988 Jul;7(4):307-10. [PubMed]
- 47.
- Ramasubbu B, James D, Scurr A, Sandilands EA. Serum alkalinisation is the cornerstone of treatment for amitriptyline poisoning. BMJ Case Rep. 2016 Apr 11;2016:10.1136/bcr-2016-214685. [PMC free article] [PubMed]
- 48.
- Woolf AD, Erdman AR, Nelson LS, Caravati EM, Cobaugh DJ, Booze LL, Wax PM, Manoguerra AS, Scharman EJ, Olson KR, Chyka PA, Christianson G, Troutman WG., American Association of Poison Control Centers. Tricyclic antidepressant poisoning: an evidence-based consensus guideline for out-of-hospital management. Clin Toxicol (Phila). 2007;45(3):203-33. [PubMed]
- 49.
- Tran TP, Panacek EA, Rhee KJ, Foulke GE. Response to dopamine vs norepinephrine in tricyclic antidepressant-induced hypotension. Acad Emerg Med. 1997 Sep;4(9):864-8. [PubMed]
- 50.
- Kerr GW, McGuffie AC, Wilkie S. Tricyclic antidepressant overdose: a review. Emerg Med J. 2001 Jul;18(4):236-41. [PMC free article] [PubMed]
- 51.
- Rudorfer MV, Potter WZ. Metabolism of tricyclic antidepressants. Cell Mol Neurobiol. 1999 Jun;19(3):373-409. [PubMed]
Tricyclic antidepressants and tetracyclic antidepressants
Tricyclic and tetracyclic antidepressants affect brain chemicals to ease depression symptoms. Explore their possible side effects and whether one of these antidepressants may be a good option for you.
Tricyclic and tetracyclic antidepressants, also called cyclic antidepressants, are among the earliest antidepressants developed. They’re effective, but they’ve generally been replaced by antidepressants that cause fewer side effects. However, cyclic antidepressants may be a good option for some people. In certain cases, they relieve depression when other treatments have failed.
Cyclic antidepressants are designated as tricyclic or tetracyclic, depending on the number of rings in their chemical structure — three (tri) or four (tetra).
How cyclic antidepressants work
Cyclic antidepressants ease depression by affecting chemical messengers (neurotransmitters) used to communicate between brain cells. Like most antidepressants, cyclic antidepressants work by ultimately effecting changes in brain chemistry and communication in brain nerve cell circuitry known to regulate mood, to help relieve depression.
Cyclic antidepressants block the reabsorption (reuptake) of the neurotransmitters serotonin (ser-o-TOE-nin) and norepinephrine (nor-ep-ih-NEF-rin), increasing the levels of these two neurotransmitters in the brain. Cyclic antidepressants also affect other chemical messengers, which can lead to a number of side effects.
Cyclic antidepressants approved to treat depression
The Food and Drug Administration (FDA) approved these tricyclic antidepressants to treat depression:
- Amitriptyline
- Amoxapine
- Desipramine (Norpramin)
- Doxepin
- Imipramine (Tofranil)
- Nortriptyline (Pamelor)
- Protriptyline
- Trimipramine
The FDA approved the tetracycline antidepressant maprotiline to treat depression.
Sometimes cyclic antidepressants are used to treat conditions other than depression, such as obsessive-compulsive disorder, anxiety disorders or nerve-related (neuropathic) pain.
Possible side effects and cautions
Because of the different ways cyclic antidepressants work, side effects vary somewhat from medication to medication. Some side effects may go away after a time, while others may lead you and your doctor to try a different medication. Side effects may also be dependent on the dose, with higher doses often causing more side effects.
Some common possible side effects include:
- Drowsiness
- Blurred vision
- Constipation
- Dry mouth
- Drop in blood pressure when moving from sitting to standing, which can cause lightheadedness
- Urine retention
Other possible side effects include:
- Weight loss
- Increased appetite leading to weight gain
- Excessive sweating
- Tremor
- Sexual problems, such as difficulty achieving an erection, delayed orgasm or low sex drive
Generally speaking:
- Amitriptyline, doxepin, imipramine and trimipramine are more likely to make you sleepy than other tricyclic antidepressants are. Taking these medications at bedtime may help.
- Amitriptyline, doxepin, imipramine and trimipramine are more likely to cause weight gain than other tricyclic antidepressants are.
- Nortriptyline and desipramine appear to have better tolerated side effects than other tricyclic antidepressants do.
For antidepressants that cause sleepiness, be careful about doing activities that require you to be alert, such as driving a car, until you know how the medication will affect you.
Which antidepressant is best for you depends on a number of issues, such as your symptoms and any other health conditions you may have. Ask your doctor and pharmacist about the most common possible side effects for your specific antidepressant and read the patient medication guide that comes with the prescription.
Safety issues
Some tricyclic antidepressants are more likely to cause side effects that affect safety, such as:
- Disorientation or confusion, particularly in older people when the dosage is too high
- Increased or irregular heart rate
- More-frequent seizures in people who have seizures
Other issues to discuss with your doctor before you take a cyclic antidepressant:
- Antidepressants and pregnancy. Talk to your doctor about the risks and benefits of using specific antidepressants. Some antidepressants may harm your baby if you take them during pregnancy or while you’re breast-feeding. If you’re taking an antidepressant and you’re considering getting pregnant, talk to your doctor or mental health professional about the possible risks. Don’t stop taking your medication without contacting your doctor first, as stopping might pose risks for you.
- Drug interactions. When taking an antidepressant, tell your doctor about any other prescription or over-the-counter medications, herbs or other supplements you’re taking. Some antidepressants can cause dangerous reactions when combined with certain medications or herbal supplements.
- Serotonin syndrome. Rarely, an antidepressant can cause high levels of serotonin to accumulate in your body. Serotonin syndrome most often occurs when two medications that raise the level of serotonin are combined. These include other antidepressants, certain pain or headache medications, and the herbal supplement St. John’s wort.
- Signs and symptoms of serotonin syndrome include anxiety, agitation, high fever, sweating, confusion, tremors, restlessness, lack of coordination, major changes in blood pressure and a rapid heart rate.
- Seek immediate medical attention if you have any of these signs and symptoms.
- Safety and blood tests. Your doctor may recommend blood levels to determine the most effective dose. Some side effects and benefits of cyclic antidepressants depend on the dose. Overdose of cyclic antidepressants can be dangerous.
- Chronic health conditions. Cyclic antidepressants can cause problems in people with certain health conditions. For example, if you have glaucoma, an enlarged prostate, heart problems, diabetes, liver disease or a history of seizures, talk to your doctor about whether a cyclic antidepressant is a safe choice for you.
Suicide risk and antidepressants
Most antidepressants are generally safe, but the FDA requires that all antidepressants carry black box warnings, the strictest warnings for prescriptions. In some cases, children, teenagers and young adults under 25 may have an increase in suicidal thoughts or behavior when taking antidepressants, especially in the first few weeks after starting or when the dose is changed.
Anyone taking an antidepressant should be watched closely for worsening depression or unusual behavior. If you or someone you know has suicidal thoughts when taking an antidepressant, immediately contact your doctor or get emergency help.
Keep in mind that antidepressants are more likely to reduce suicide risk in the long run by improving mood.
Stopping treatment with cyclic antidepressants
Cyclic antidepressants aren’t considered addictive. However, stopping antidepressant treatment abruptly or missing several doses can cause withdrawal-like symptoms. Symptoms may vary depending on how the drug works. This is sometimes called discontinuation syndrome. Work with your doctor to gradually and safely decrease your dose.
Withdrawal-like symptoms can include:
- Agitation, irritability or anxiety
- Nausea
- Sweating
- Flu-like symptoms, such as chills and muscle aches
- Insomnia
- Lethargy
- Headache
Finding the right antidepressant
People may react differently to the same antidepressant. For example, a particular drug may work better — or not as well — for you than for another person. Or you may have more, or fewer, side effects from taking a specific antidepressant than someone else does.
Inherited traits may play a role in how antidepressants affect you. In some cases, where available, results of special blood tests may offer clues about how your body may respond to a specific antidepressant. However, other variables besides genetics can affect your response to medication.
When choosing an antidepressant, your doctor takes into account your symptoms, any health problems, other medications you take, and what’s worked for you in the past.
Typically, it may take several weeks or longer before an antidepressant is fully effective and for initial side effects to ease up. Your doctor may recommend dose adjustments or different antidepressants, but with patience, you and your doctor can find a medication that works well for you.








