Warfarin is an oral anticoagulant commonly used to treat and prevent blood clots. Warfarin has multiple FDA-approved and off-label clinical uses. FDA-approved clinical uses for warfarin: Prophylaxis and treatment of venous thrombosis and arising pulmonary embolisms.
Warfarin is a commonly used anticoagulant (often referred to as a “blood thinner”) that helps prevent blood clot formation. It works by inhibiting the production of vitamin K-dependent clotting factors, which are essential for the blood clotting process. Although warfarin does not literally “thin” the blood, it reduces the blood’s ability to form clots.
Main Uses of Warfarin:
Warfarin is prescribed to prevent and treat conditions related to abnormal blood clotting, including:
- Deep Vein Thrombosis (DVT): A blood clot that forms in a deep vein, usually in the legs. DVT can be dangerous if the clot breaks loose and travels to the lungs.
- Pulmonary Embolism (PE): A blockage in the lung’s arteries, often caused by a blood clot that travels from the legs (DVT) to the lungs. This can be life-threatening if not treated promptly.
- Atrial Fibrillation (AFib): An irregular heart rhythm that increases the risk of blood clots forming in the heart. These clots can travel to the brain, causing a stroke. Warfarin is commonly used to reduce the risk of stroke in patients with AFib.
- Heart Valve Replacement: After heart valve replacement surgery, warfarin is often prescribed to prevent clots from forming on or around the artificial heart valve.
- Stroke Prevention: In people at high risk for clot formation, such as those with AFib or a history of prior strokes or blood clots, warfarin is used to prevent new clots from forming.
Medical Uses of Warfarin
Warfarin is used to decrease the tendency for thrombosis, or as secondary prophylaxis (prevention of further episodes) in those individuals who have already formed a blood clot (thrombus). Warfarin treatment can help prevent formation of future blood clots and help reduce the risk of embolism (migration of a thrombus to a spot where it blocks blood supply to a vital organ).
Warfarin is best suited for anticoagulation (clot formation inhibition) in areas of slowly running blood (such as in veins and the pooled blood behind artificial and natural valves), and in blood pooled in dysfunctional cardiac atria. Thus, common clinical indications for warfarin use are atrial fibrillation, the presence of artificial heart valves, deep venous thrombosis, and pulmonary embolism (where the embolized clots first form in veins). Warfarin is also used in antiphospholipid syndrome. It has been used occasionally after heart attacks (myocardial infarctions), but is far less effective at preventing new thromboses in coronary arteries. Prevention of clotting in arteries is usually undertaken with antiplatelet drugs, which act by a different mechanism from warfarin (which normally has no effect on platelet function). It can be used to treat people following ischemic strokes due to atrial fibrillation, though direct oral anticoagulants (DOACs) may offer greater benefits.
How Warfarin Works:
Warfarin acts by interfering with the action of vitamin K, which is necessary for the synthesis of clotting factors in the liver. These clotting factors (II, VII, IX, and X) help form blood clots to stop bleeding. By reducing the production of these clotting factors, warfarin slows down the body’s clotting ability, which helps prevent clots from forming or growing.
Monitoring Warfarin Therapy:
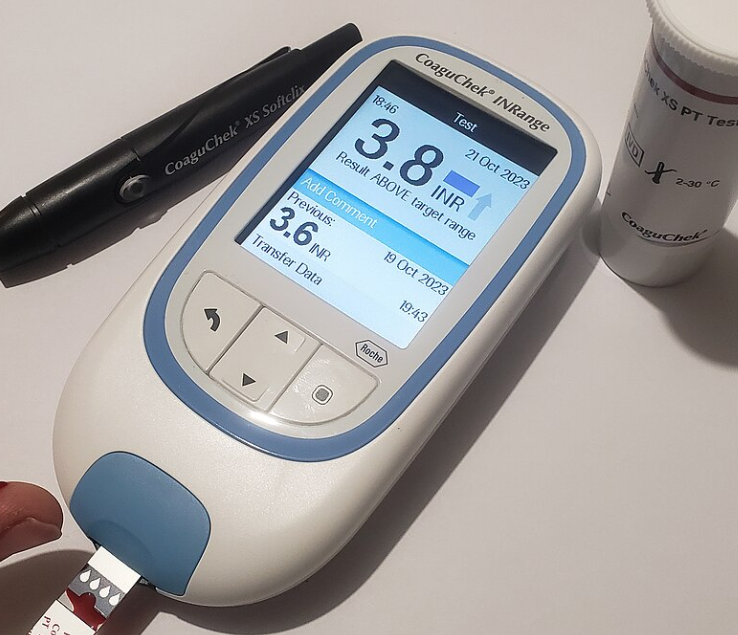
One of the key challenges of warfarin therapy is maintaining the correct balance between preventing clots and avoiding excessive bleeding. To ensure safety, warfarin patients must regularly monitor their International Normalized Ratio (INR), a blood test that measures the time it takes for blood to clot. The INR helps determine the appropriate dosage:
- A target INR range is usually between 2.0 and 3.0 for most conditions.
- A higher INR indicates increased bleeding risk, while a lower INR means there’s a higher risk of clot formation.
Side Effects of Warfarin:
Warfarin is effective but comes with some potential risks, the most significant being increased bleeding. Common side effects include:
- Bleeding: The most serious side effect of warfarin is excessive bleeding, which can occur in various forms:
- Nosebleeds
- Gum bleeding
- Bruising more easily than usual
- Blood in the urine (hematuria)
- Black or tarry stools (indicating internal bleeding)
- Severe or prolonged bleeding from cuts or injuries
- Gastrointestinal bleeding or brain hemorrhage (less common but serious risks), particularly in patients with other risk factors like high blood pressure, peptic ulcers, or history of falls.
- Skin necrosis or gangrene: This is a very rare but serious condition where the skin or other tissues die due to blood clots forming in small blood vessels.
Food and Drug Interactions:
Warfarin has many interactions with foods, drugs, and even supplements, which can affect its effectiveness:
- Foods high in vitamin K can reduce the effect of warfarin, making it less effective in preventing blood clots. Foods rich in vitamin K include:
- Green leafy vegetables (spinach, kale, broccoli, Brussels sprouts)
- Certain oils (like soybean and canola oil) Patients are often advised to maintain a consistent intake of these foods to avoid fluctuating INR levels.
- Alcohol: Excessive alcohol consumption can increase the risk of bleeding when on warfarin.
- Medications: Many prescription and over-the-counter medications interact with warfarin:
- Other anticoagulants: Combining warfarin with other blood thinners or anticoagulants can significantly increase the risk of bleeding.
Monitoring and Dosage Adjustment:
Because of its narrow therapeutic range, warfarin dosage needs careful adjustment based on regular INR monitoring:
- Too high an INR (above 3.0) increases the risk of bleeding.
- Too low an INR (below 2.0) may not provide sufficient protection against clotting.
Special Considerations:
- Pregnancy: Warfarin is generally contraindicated during pregnancy, as it can cross the placenta and cause birth defects or bleeding in the unborn baby. Safer alternatives like heparin are often used instead.
- Liver and Kidney Disease: Patients with liver or kidney disease need closer monitoring, as these organs play a crucial role in the metabolism and clearance of warfarin.
- Falls and Injuries: Since warfarin increases the risk of bleeding, individuals at risk of frequent falls or injuries should take special precautions to avoid accidents that could lead to serious bleeding complications.
- Dental or Surgical Procedures: Patients taking warfarin often need to stop or adjust their dosage before surgery or dental procedures to reduce the risk of bleeding, under a doctor’s supervision.
Osteoporosi
After initial reports that warfarin could reduce bone mineral density, several studies demonstrated a link between warfarin use and osteoporosis-related fracture. A 1999 study in 572 women taking warfarin for deep venous thrombosis, risk of vertebral fracture and rib fracture was increased; other fracture types did not occur more commonly. A 2002 study looking at a randomly selected selection of 1,523 patients with osteoporotic fracture found no increased exposure to anticoagulants compared to controls, and neither did stratification of the duration of anticoagulation reveal a trend towards fracture.
A 2006 retrospective study of 14,564 Medicare recipients showed that warfarin use for more than one year was linked with a 60% increased risk of osteoporosis-related fracture in men, but no association in women was seen. The mechanism was thought to be a combination of reduced intake of vitamin K (a vitamin necessary for bone health) and inhibition by warfarin of vitamin K-mediated carboxylation of certain bone proteins, rendering them nonfunctional.
Conclusion:
Warfarin is an effective anticoagulant that has saved countless lives by preventing blood clots, strokes, and other thrombotic events. However, due to its narrow therapeutic window, potential for interactions, and risk of serious bleeding, it requires careful management and regular INR monitoring. Always consult a healthcare provider before making any changes to your diet, medications, or warfarin dosage.