Even though aspirin and Ibuprofen are both NSAIDs (nonsteroidal anti-inflammatory drugs) and work similarly, that is by blocking the body’s production of prostaglandins which relieves pain and inflammation, there are several differences between the two drugs and they are not considered interchangeable.
Aspirin and ibuprofen are two of the most widely used over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs). While they share similarities in their ability to reduce pain, inflammation, and fever, they differ in several key aspects, including their chemical structures, mechanisms of action, uses, side effects, and other pharmacological properties. This comprehensive comparison aims to elucidate these differences to provide a clear understanding of each medication.
1. Chemical Structure and Classification
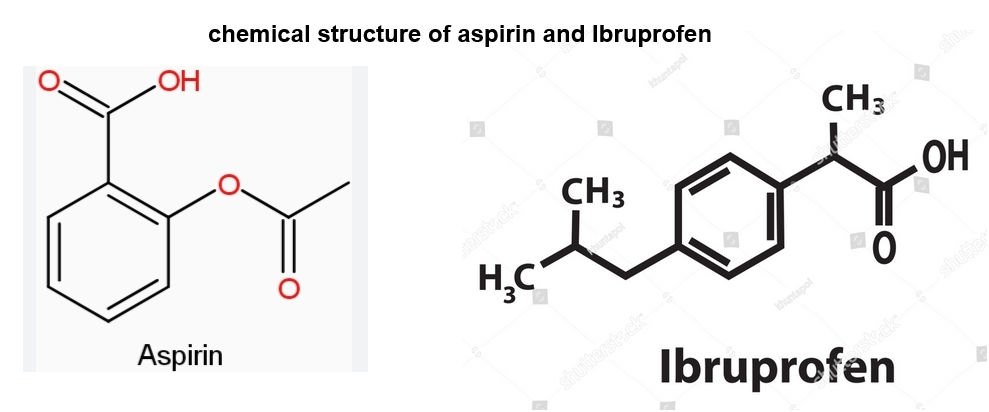
- Aspirin (Acetylsalicylic Acid)
- Chemical Structure: Aspirin is derived from salicylic acid and contains an acetyl group attached to the benzene ring.
- Classification: It belongs to the salicylate class of NSAIDs.
- Ibuprofen
- Chemical Structure: Ibuprofen is a propionic acid derivative with a chiral center, existing in two enantiomeric forms (S- and R-ibuprofen).
- Classification: It is classified as a propionic acid NSAID.
Key Difference: While both are NSAIDs, aspirin is a salicylate, and ibuprofen belongs to the propionic acid class, leading to differences in their pharmacological profiles.
2. Mechanism of Action
Both aspirin and ibuprofen exert their effects by inhibiting cyclooxygenase (COX) enzymes, which play a crucial role in the synthesis of prostaglandins and thromboxanes—mediators of inflammation, pain, and platelet aggregation.
- Aspirin:
- Ibuprofen:
- Reversible Inhibition: Ibuprofen reversibly inhibits both COX-1 and COX-2 enzymes.
- Shorter Duration: Its effects on platelet function are temporary, as the enzyme activity can resume once ibuprofen is cleared from the system.
Key Difference: Aspirin causes irreversible COX inhibition, leading to prolonged antiplatelet effects, whereas ibuprofen’s inhibition is reversible and short-lived.
3. Indications and Uses
- Aspirin:
- Pain Relief: Effective for mild to moderate pain such as headaches, muscle aches, and arthritis.
- Anti-inflammatory: Used in inflammatory conditions like rheumatoid arthritis.
- Antipyretic: Reduces fever.
- Cardiovascular Protection: Low-dose aspirin is prescribed to prevent myocardial infarction, ischemic stroke, and other cardiovascular events due to its antiplatelet effects.
- Prevention of Certain Cancers: Some studies suggest a role in reducing the risk of colorectal cancer.
- Ibuprofen:
- Pain Relief: Similar to aspirin, used for headaches, dental pain, menstrual cramps, muscle aches, and arthritis.
- Anti-inflammatory: Effective in reducing inflammation in conditions like rheumatoid arthritis and osteoarthritis.
- Antipyretic: Lowers fever.
- Use in Children: Often used in pediatric populations for fever and pain management.
Key Difference: While both are used for pain, fever, and inflammation, aspirin has a unique role in cardiovascular protection and cancer prevention, which ibuprofen does not.
4. Dosage and Administration
- Aspirin:
- Adult Dosage for Pain/Fever: Typically 325-650 mg every 4-6 hours as needed, not exceeding 4,000 mg per day.
- Low-Dose for Cardiovascular Protection: 81-325 mg daily.
- Administration: Can be taken with or without food, but taking with food may reduce gastrointestinal discomfort.
- Ibuprofen:
- Adult Dosage for Pain/Fever: Usually 200-400 mg every 4-6 hours as needed, not exceeding 3,200 mg per day.
- Pediatric Dosage: Varies based on weight and age; typically 5-10 mg/kg every 6-8 hours.
- Administration: Best taken with food or milk to minimize stomach upset.
Key Difference: Ibuprofen is often dosed more frequently with a higher maximum daily dose for over-the-counter use, whereas aspirin has specific low-dose regimens for cardiovascular purposes.
5. Pharmacokinetics
- Aspirin:
- Absorption: Rapidly absorbed from the stomach and upper intestine.
- Distribution: Widely distributed throughout the body tissues.
- Metabolism: Metabolized in the liver to salicylic acid and other metabolites.
- Excretion: Primarily excreted by the kidneys.
- Half-Life: Approximately 3-4 hours for immediate-release forms; the antiplatelet effect lasts for the lifespan of platelets (7-10 days).
- Ibuprofen:
- Absorption: Quickly absorbed from the gastrointestinal tract.
- Distribution: Extensively binds to plasma proteins (about 99%).
- Metabolism: Primarily metabolized in the liver to inactive metabolites.
- Excretion: Excreted unchanged and as metabolites via the kidneys.
- Half-Life: Approximately 2-4 hours.
Key Difference: Both have similar absorption profiles, but aspirin’s antiplatelet effect lasts much longer due to irreversible enzyme inhibition, whereas ibuprofen’s effects are shorter-lived.
6. Side Effects and Adverse Reactions
- Aspirin:
- Gastrointestinal: Risk of stomach ulcers, bleeding, and gastritis.
- Bleeding Risk: Increased bleeding tendency due to antiplatelet effects.
- Allergic Reactions: Can cause asthma exacerbation, especially in aspirin-sensitive individuals.
- Reye’s Syndrome: Risk in children and adolescents with viral infections.
- Other: Tinnitus at high doses.
- Ibuprofen:
- Gastrointestinal: Risk of stomach upset, ulcers, and bleeding, though generally lower than aspirin.
- Cardiovascular: Long-term use may increase the risk of heart attack and stroke.
- Renal: Can cause kidney impairment, especially with prolonged use or in dehydrated individuals.
- Allergic Reactions: Can cause skin rashes and, in rare cases, severe hypersensitivity reactions.
- Other: May cause dizziness or headache.
Key Difference: Both have gastrointestinal risks, but aspirin has a unique risk of Reye’s syndrome in children and a more pronounced antiplatelet-related bleeding risk.

7. Contraindications and Precautions
- Aspirin:
- Contraindications:
- Children and teenagers with viral infections (due to Reye’s syndrome risk).
- Active peptic ulcer disease.
- Hemorrhagic disorders.
- Hypersensitivity to aspirin or other NSAIDs.
- Precautions:
- Use with caution in individuals with asthma, liver or kidney disease, or bleeding disorders.
- Not recommended during pregnancy, especially in the third trimester.
- Contraindications:
- Ibuprofen:
- Contraindications:
- Active gastrointestinal bleeding or ulcers.
- Severe heart failure.
- Hypersensitivity to ibuprofen or other NSAIDs.
- Third trimester of pregnancy.
- Precautions:
- Caution in individuals with hypertension, heart disease, kidney or liver impairment.
- Not recommended for prolonged use without medical supervision.
- Contraindications:
Key Difference: Aspirin is contraindicated in children with viral infections due to Reye’s syndrome, a concern not applicable to ibuprofen.

8. Drug Interactions
- Aspirin:
- Anticoagulants: Increased risk of bleeding when taken with warfarin or other blood thinners.
- Other NSAIDs or Corticosteroids: Heightened risk of gastrointestinal bleeding.
- ACE Inhibitors and Diuretics: May reduce the efficacy of antihypertensive medications.
- SSRIs: Enhanced bleeding risk when combined with selective serotonin reuptake inhibitors.
- Ibuprofen:
- Anticoagulants: Similar increased bleeding risk as aspirin.
- Antihypertensives: Can reduce the effectiveness of ACE inhibitors, beta-blockers, and diuretics.
- Lithium and Methotrexate: Ibuprofen can increase serum levels, leading to toxicity.
- SSRIs: Increased risk of gastrointestinal bleeding.
Key Difference: Both interact with anticoagulants and antihypertensives, but aspirin’s antiplatelet action may have more pronounced interactions related to bleeding risk.
9. Special Considerations
- Use in Children:
- Aspirin: Generally avoided in children and teenagers with viral infections due to the risk of Reye’s syndrome.
- Ibuprofen: Commonly used for pain and fever in pediatric populations, with appropriate dosing based on weight and age.
- Pregnancy:
- Aspirin: Generally avoided, especially in the third trimester, due to risks to the fetus and potential complications during delivery.
- Ibuprofen: Also avoided in the third trimester; earlier trimesters require medical consultation before use.
- Elderly Population:
- Both medications require caution due to increased risk of gastrointestinal bleeding, renal impairment, and interactions with other medications.
Key Difference: Aspirin has a specific contraindication in children and teenagers with viral infections, a concern not present with ibuprofen.
10. Over-the-Counter Availability and Brand Names
- Aspirin:
- Availability: Widely available over-the-counter in various formulations, including tablets, enteric-coated tablets, and powders.
- Common Brand Names: Bayer Aspirin, Bufferin, Ecotrin.
- Ibuprofen:
- Availability: Over-the-counter in tablets, capsules, liquid suspensions, and chewable forms.
- Common Brand Names: Advil, Motrin, Nurofen.
Key Difference: Both are readily available OTC, but brand names differ, and aspirin is often found in low-dose formulations specifically for cardiovascular use.
11. Historical Background
- Aspirin:
- Development: Synthesized in 1897 by Felix Hoffmann at Bayer as a less irritating form of salicylic acid.
- Historical Use: Used for over a century for pain, fever, and inflammation; recognized for its cardiovascular benefits in the latter half of the 20th century.
- Ibuprofen:
- Development: First synthesized in the 1960s by Dr. Stewart Adams and his team at Boots UK.
- Historical Use: Introduced to the market in the 1970s, became popular in the 1980s as an effective OTC pain reliever with fewer gastrointestinal side effects compared to aspirin.
Key Difference: Aspirin has a longer history of use, dating back to ancient times in various forms, while ibuprofen is a relatively newer NSAID developed in the mid-20th century.
12. Conclusion
The main differences between aspirin and ibuprofen are:
- Aspirin is significantly more likely than low-dose ibuprofen to cause gastrointestinal side effects. The risk of other side effects is similar
- Aspirin should not be used in children under 12 years of age or those under the age of 16 with a viral illness because of the risk of Reye’s syndrome. Ibuprofen is approved for use in children over the age of 6 months and may be given to children with a viral illness
- Aspirin may be used at a low dose to reduce the risk of a heart attack or stroke or to prevent blood clotting. Ibuprofen has less of an effect on blood cells or platelets so is not used for this indication
- Aspirin is also a salicylate because it is derived from salicylic acid. Some people are sensitive to salicylates; symptoms may include asthma-like reactions, nasal congestion, and hives
- Ibuprofen is preferred over aspirin for ongoing conditions such as arthritis, menstrual cramps, and back pain. This is because the risk of gastrointestinal side effects increases the longer the duration of treatment and the risk of GI effects associated with aspirin use is already high. Aspirin may be used on an occasional basis to treat headaches, minor body aches, and tooth pain
- Aspirin use does not appear to be associated with a higher risk of cardiovascular events, nor does low-dose ibuprofen (up to 1200mg/day). However, high-dose ibuprofen (1200mg to 2400mg/day) is associated with a higher risk. People with a history of heart disease or stroke should use NSAIDs with caution and they should not be used after coronary artery bypass graft (CABG) surgery.
Other points to note include:
- Generic aspirin is available and brand names for aspirin include Bayer Aspirin, Ecotrin, and Bufferin
- Generic ibuprofen is available and brand names for ibuprofen include Motrin and Advil
- Neither aspirin or ibuprofen is recommended during pregnancy
- People with gastrointestinal disorders, bleeding disorders or hemophiliacs should avoid aspirin and should only take ibuprofen if recommended and monitored by their doctor
- Aspirin and ibuprofen should not be taken together. If you are prescribed aspirin to reduce your risk of heart attack or stroke, talk with your doctor before taking any NSAIDs, as these may negate the protective effect of aspirin
- Both aspirin and ibuprofen may cause kidney toxicity and allergic-type reactions. Interactions are also similar, with both aspirin and ibuprofen interacting with angiotensin-II receptor blockers (ARBs), diuretics, clopidogrel, warfarin, dabigatran, and aspirin.
While aspirin and ibuprofen are both effective NSAIDs used to manage pain, inflammation, and fever, they possess distinct differences that influence their suitability for various clinical scenarios:
- Aspirin is uniquely valuable for its irreversible antiplatelet effects, making it essential in cardiovascular disease prevention. However, its use is limited in children with viral infections and requires caution in individuals at risk for gastrointestinal bleeding.
- Ibuprofen offers similar analgesic and antipyretic benefits without the long-term antiplatelet effects, making it more suitable for acute pain and inflammation management in a broader population, including children. Nonetheless, it carries risks related to cardiovascular health and renal function with prolonged use.
Choosing between aspirin and ibuprofen should consider the specific health needs, underlying conditions, potential drug interactions, and individual risk factors. It is always advisable to consult with a healthcare professional before starting or switching medications.
Pain Medications, Pain Relief, and Pain Management

?")





