The primary reason individuals seek medical attention is often due to pain.
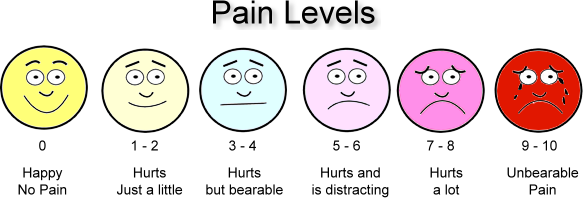
Pain itself can manifest in various ways—it may be described as sharp or dull, intermittent or constant, throbbing or steady. Describing pain can sometimes be challenging, as it may be localized to a specific area or spread across a larger region. The intensity of pain is diverse, ranging from mild discomfort to intolerable agony.
There is considerable variability among individuals in their capacity to endure pain. While one person might find it challenging to tolerate the pain from a minor cut or bruise, another individual may endure significant pain resulting from a major accident or a knife wound with minimal expression of discomfort. The ability to withstand pain is influenced by factors such as mood, personality, and the surrounding circumstances. For instance, during an intense moment of excitement in an athletic competition, an athlete may overlook a severe bruise. However, the awareness of pain is likely to be heightened after the match, especially if the team did not emerge victorious.
1. How Many Categories of Analgesics Are There ?
Analgesics are a class of medications primarily designed to relieve pain. These drugs work by targeting the nervous system and altering the perception of pain or inhibiting the inflammatory processes that lead to pain. Analgesics can be classified into various categories based on their mechanisms of action and chemical structures.
Analgesics are drugs that relieve pain. They can be classified into several categories based on their mechanisms of action and chemical structures. The main categories of analgesics include:
- Nonsteroidal Anti-Inflammatory Drugs (NSAIDs): These drugs reduce pain, inflammation, and fever by inhibiting the enzyme cyclooxygenase (COX), which is involved in the production of prostaglandins. Common examples include ibuprofen, naproxen, and aspirin.
- Acetaminophen (Paracetamol): While it has analgesic and antipyretic (fever-reducing) properties, acetaminophen’s mechanism of action is not fully understood. It is commonly used for pain relief and reducing fever. Unlike NSAIDs, it has little to no anti-inflammatory effects.
- Opioids (Narcotics): These drugs act on the central nervous system to relieve pain. They are derived from the opium poppy or synthesized to mimic its effects. Examples include morphine, codeine, oxycodone, and fentanyl. Opioids are potent pain relievers but can also be associated with side effects and the risk of dependence.
- Adjuvant Analgesics: These are drugs that were not originally developed for pain management but have been found to be effective in certain painful conditions. They include drugs such as antidepressants, anticonvulsants, and muscle relaxants.
- Local Anesthetics: These drugs block sensation in a specific area of the body, providing pain relief for a limited duration. They are commonly used in medical procedures and dental work.
2. Nonopioid Analgesics
Nonopioid analgesics are a class of pain-relieving medications that do not belong to the opioid family. Unlike opioids, which act on the central nervous system to modulate pain perception, nonopioid analgesics primarily work by blocking pain signals or reducing inflammation. The main categories of nonopioid analgesics include:
- Nonsteroidal Anti-Inflammatory Drugs (NSAIDs): These drugs, such as ibuprofen, naproxen, and aspirin, work by inhibiting the enzyme cyclooxygenase (COX), which is involved in the production of prostaglandins. Prostaglandins are chemicals that promote inflammation, pain, and fever. By reducing prostaglandin levels, NSAIDs provide pain relief and have anti-inflammatory and antipyretic (fever-reducing) effects.
- Acetaminophen (Paracetamol): Acetaminophen is a non-opioid analgesic that primarily reduces pain and fever. Its exact mechanism of action is not fully understood, but it is thought to affect the central nervous system. Unlike NSAIDs, acetaminophen has little to no anti-inflammatory effects.
- Corticosteroids: In certain situations, corticosteroids may be used as nonopioid analgesics, especially for their potent anti-inflammatory properties. They are often administered locally (topically or through injections) to target specific areas of inflammation.
- Adjuvant Analgesics: Some medications that were not originally developed for pain relief may be used as adjuvant analgesics. This category includes drugs such as certain antidepressants, anticonvulsants, and muscle relaxants, which may be effective in managing certain types of pain.
A variety of nonopioid analgesics are available. They are often effective for mild to moderate pain. These drugs are often the preferred drugs for treating pain. People do not become physically dependent on these drugs or tolerant of their pain-relieving effects.
Aspirin and acetaminophen are available without a prescription (over-the-counter, or OTC). Several other nonopioid analgesics (such as ibuprofen, ketoprofen, and naproxen) are available OTC and by prescription, usually in higher-dose formulations, with more active ingredient per dose than OTC formulations.
OTC analgesics are reasonably safe to take for short periods of time, but their labels caution against taking them for more than 7 to 10 days to treat pain. A doctor should be consulted if symptoms worsen or do not go away.
2.1 Nonsteroidal Anti-Inflammatory Drugs
Nonsteroidal Anti-Inflammatory Drugs, commonly known as NSAIDs, are a class of medications that provide pain relief, reduce inflammation, and lower fever. They achieve these effects by inhibiting the activity of enzymes called cyclooxygenases (COX), which play a key role in the production of prostaglandins. Prostaglandins are chemical messengers that contribute to inflammation, pain, and fever. By blocking COX and reducing prostaglandin levels, NSAIDs alleviate these symptoms.
There are two main types of cyclooxygenases: COX-1 and COX-2. COX-1 is involved in maintaining the normal lining of the stomach and intestines, while COX-2 is induced in response to injury and inflammation. Traditional NSAIDs, such as ibuprofen, naproxen, and aspirin, inhibit both COX-1 and COX-2, which can lead to gastrointestinal side effects.
Common examples of NSAIDs include:
- Ibuprofen: Available over-the-counter and by prescription, ibuprofen is commonly used for pain relief, inflammation reduction, and fever reduction. Brand names include Advil and Motrin.
- Naproxen: Similar to ibuprofen, naproxen is available over-the-counter and by prescription. It has a longer duration of action than ibuprofen and is sold under brand names such as Aleve.
- Aspirin (Acetylsalicylic Acid): Aspirin not only has analgesic and anti-inflammatory properties but also has antipyretic (fever-reducing) effects. It is available over-the-counter and is often used for pain relief and as a blood thinner. Aspirin has a unique feature of irreversibly inhibiting platelets, which can provide cardiovascular benefits.
- Diclofenac: Available in various formulations, including oral tablets, topical gels, and eye drops. It is used to treat pain, inflammation, and joint stiffness caused by conditions such as osteoarthritis and rheumatoid arthritis.
- Celecoxib: This is a selective COX-2 inhibitor, meaning it primarily targets cyclooxygenase-2 without affecting COX-1 to the same extent. Celecoxib is often prescribed for conditions like osteoarthritis, rheumatoid arthritis, and ankylosing spondylitis. It may have a lower risk of causing gastrointestinal side effects compared to non-selective NSAIDs.
- Meloxicam: A long-acting NSAID used for the treatment of osteoarthritis and rheumatoid arthritis. It is available in oral form and may be taken once daily.
- Indomethacin: Known for its potent anti-inflammatory effects, indomethacin is used to manage conditions such as gout, arthritis, and certain types of bursitis. It is available in oral and rectal forms.
- Ketorolac: Often used for short-term relief of moderate to severe pain, such as that following surgery. Ketorolac is available in both oral and injectable forms. It’s important to note that prolonged use of injectable forms is generally avoided due to the risk of kidney damage.
- Piroxicam: An NSAID that is longer-acting than some others, requiring once-daily dosing. It is used for the treatment of various inflammatory conditions.
- Etodolac: This NSAID is used to relieve pain and reduce inflammation associated with osteoarthritis and rheumatoid arthritis. It is available in oral form.
- Nabumetone: A prodrug that is converted to an active form in the body, nabumetone is used for the relief of pain and inflammation associated with osteoarthritis and rheumatoid arthritis.
- Oxaprozin: An NSAID used for the management of osteoarthritis and rheumatoid arthritis. It is typically taken orally.
Most nonopioid analgesics are classified as nonsteroidal anti-inflammatory drugs (NSAIDs). NSAIDs are used to treat mild to moderate pain and may be combined with opioids to treat moderate to severe pain. NSAIDs not only relieve pain, but they may also reduce the inflammation that often accompanies and worsens pain. However, to reduce inflammation, NSAIDs usually need to be taken at high doses and for a relatively long time.
All NSAIDs can be taken by mouth. Two NSAIDs, ketorolac and diclofenac, can also be given by injection into a vein (intravenously) or muscle (intramuscularly). Indomethacin can be given by a suppository inserted in the rectum. Diclofenac is also available as a cream.
Although widely used, NSAIDs can have side effects, sometimes serious ones.
Problems in the digestive tract: All NSAIDs tend to irritate the stomach’s lining and cause digestive upset (such as heartburn, indigestion, nausea, bloating, diarrhea, and stomach pain), peptic ulcers, and bleeding in the digestive tract (gastrointestinal bleeding). Coxibs (COX-2 inhibitors) are less likely to irritate the stomach and cause bleeding than other NSAIDs. However, if people take a coxib and aspirin, these problems are just as likely. Taking NSAIDs with food and using antacids may help prevent stomach irritation. The drug misoprostol can help prevent stomach irritation and ulcers, but it can cause other problems, including diarrhea. Proton pump inhibitors (such as omeprazole) or histamine-2 (H2) blockers (such as famotidine), which are used to treat peptic ulcers, can also help prevent stomach problems due to NSAIDs.
Bleeding problems: All NSAIDs interfere with the clotting tendency of platelets (cell-like particles in the blood that help stop bleeding when blood vessels are injured). Consequently, NSAIDs increase the risk of bleeding, especially in the digestive tract if they also irritate the stomach’s lining. Coxibs are less likely to cause bleeding than other NSAIDs.
Problems related to retaining fluids: NSAIDs sometimes cause fluid retention and swelling. Regular use of NSAIDs may also increase the risk of developing a kidney disorder, sometimes resulting in kidney failure (a disorder called analgesic nephropathy).
Increased risk of heart and blood vessel disorders: Studies suggest that with all NSAIDs except aspirin, the risk of heart attack, stroke, and blood clots in the legs may be increased. The risk appears to be higher with higher doses and longer use of the drug. The risk is also higher with some NSAIDs than with others. These problems may be related directly to the drug’s effect on clotting or indirectly to a small but persistent increase in blood pressure caused by the drug.
Taking NSAIDs for a short time is unlikely to cause serious problems. If people take NSAIDs for a long time, problems are more likely to occur. Such people need to have regular appointments with their doctor to check for high blood pressure, kidney failure, and ulcers or bleeding in the digestive tract and to evaluate their risk of heart disease and stroke.
The risk of side effects may be increased for some groups of people, such as the following:
For older people, the risk of side effects due to NSAIDs, particularly indomethacin and ketorolac, is increased.
For people who drink alcoholic beverages regularly and take NSAIDs, the risk of digestive upset, ulcers, and liver damage may be increased.
For people with coronary artery disease, other heart and blood vessel (cardiovascular) disorders, or risk factors for these disorders, the risk of heart attacks and stroke may be higher.
Older people and people who have heart failure, high blood pressure, or a kidney or liver disorder require a doctor’s supervision when they take NSAIDs. Some prescription heart and blood pressure drugs may not work as well when taken with these analgesics.
NSAIDs vary in how quickly they work and how long they relieve pain. Although NSAIDs are about equally effective, people respond to them differently. One person may find a particular drug to be more effective or to have fewer side effects than another.
2.2 Aspirin
Aspirin (acetylsalicylic acid) has been used for about 100 years. Aspirin is taken by mouth and provides 4 to 6 hours of moderate pain relief.
Because aspirin can irritate the stomach, it may be combined with an antacid (in a buffered product) to reduce this effect. The antacid creates an alkaline environment that helps aspirin dissolve and may reduce the time aspirin is in contact with the stomach lining. However, buffered aspirin can still irritate the stomach because aspirin also reduces the production of substances that help protect the stomach’s lining. These substances are a type of prostaglandin, which is similar to hormones.
Enteric-coated aspirin is designed to pass through the stomach intact and dissolve in the small intestine, thus minimizing direct irritation of the stomach. (Enteric refers to the small intestine.) However, enteric-coated aspirin may be absorbed erratically. If food and enteric-coated aspirin are ingested at about the same time, the aspirin is not absorbed as quickly because food delays the emptying of the stomach. Consequently, pain relief is delayed.
Aspirin increases the risk of bleeding throughout the body because it makes platelets—cell fragments in the blood that help blood clot—less able to do so. People who bruise easily may be especially vulnerable to this effect. Anyone who has ever had a bleeding disorder or uncontrolled high blood pressure should not take aspirin except under a doctor’s supervision. People who take aspirin and anticoagulants (such as warfarin) are closely monitored to avoid life-threatening bleeding. (Anticoagulants also interfere with blood clotting.) Usually, aspirin should not be taken in the week before scheduled surgery.
Aspirin can aggravate asthma. People with nasal polyps are likely to develop wheezing if they take aspirin. A few people, who are sensitive (allergic) to aspirin, may have a severe allergic reaction (anaphylaxis), leading to a rash, itching, severe breathing problems, or shock. Such a reaction requires immediate medical attention.
In very high doses, aspirin can have serious side effects such as abnormal breathing, fever, or confusion. One of the first signs of an overdose may be noise in the ears (tinnitus).
Most children and teenagers should not take aspirin because they could develop Reye syndrome if they have or have just gotten over influenza or chickenpox. Although rare, Reye syndrome can have serious consequences, including death.
2.3 Topical NSAIDs
Some NSAIDs are available as creams or gels that are applied directly to the skin over the painful area. For example, diclofenac can be applied to a joint to relieve pain due to osteoarthritis and help improve movement. Diclofenac is also available as a patch, which can be used to relieve acute pain due to minor sprains, strains, and bruises.
NSAIDs such as ibuprofen, ketoprofen, and naproxen are generally believed to be gentler on the stomach than aspirin, although few studies have compared the drugs. Like aspirin, these drugs can cause digestive upset, ulcers, and gastrointestinal bleeding. They can make asthma worse and increase blood pressure. Taking one of these drugs probably slightly increases the risk of stroke, heart attack, and blood clots in the arteries of the legs. The risk may be lower with naproxen than with other NSAIDs. Thus, naproxen may be a better choice when people with a high risk of these disorders require NSAIDs.
Although ibuprofen, ketoprofen, and naproxen generally interfere with blood clotting less than aspirin does, people should not take these drugs with anticoagulants (such as warfarin) except under a doctor’s close supervision.
People who are allergic to aspirin may also be allergic to ibuprofen, ketoprofen, and naproxen. If a rash, itching, breathing problems, or shock develops, medical attention is required immediately.
Coxibs, such as celecoxib, differ from other NSAIDs. Other NSAIDs block the following two enzymes:
COX-1, which is involved in the production of prostaglandins that protect the stomach and play a crucial role in blood clotting
COX-2, which is involved in the production of prostaglandins that promote inflammation
Coxibs tend to block mainly COX-2 enzymes. Thus, coxibs are as effective as other NSAIDs in the treatment of pain and inflammation. But coxibs are less likely to damage the stomach and to cause nausea, bloating, heartburn, bleeding, and peptic ulcers. They are also less likely to interfere with clotting than are other NSAIDs.
Because of these differences, coxibs may be useful for people who cannot tolerate other NSAIDs and for people who are at high risk of certain complications (such as gastrointestinal bleeding) from use of other NSAIDs. Such people include the following:
Older people
People who are taking anticoagulants
Those who have a history of ulcers
Those who must take an analgesic for a long time
However, coxibs, like other NSAIDs, appear to increase the risk of heart attack, stroke, and blood clots in the legs. As a result, before people with certain conditions are given a coxib, they are told about the risk and the need to be closely monitored. These conditions include
Cardiovascular disorders (such as coronary artery disease)
Strokes
Risk factors for these disorders
Coxibs, like other NSAIDs, are not appropriate for people who have heart failure or who are at increased risk of heart failure (such as those who have had a heart attack).

2.4 Acetaminophen
Acetaminophen is roughly comparable to aspirin in its potential to relieve pain and lower a fever.
But unlike NSAIDs, acetaminophen has the following characteristics:
Has virtually no useful anti-inflammatory activity
Does not affect the blood’s ability to clot
Has almost no adverse effects on the stomach
How acetaminophen works is not clearly understood.
Acetaminophen is taken by mouth or a suppository inserted into the rectum, and its effects generally last 4 to 6 hours.
Acetaminophen appears to be a very safe drug. However, high doses can lead to liver damage, which may be irreversible. People with a liver disorder should use lower doses than those usually prescribed. Whether lower doses taken for a long time can harm the liver is less certain. People who regularly consume large amounts of alcohol are probably at highest risk of liver damage from overuse of acetaminophen. People who are taking acetaminophen and stop eating because of a bad cold, influenza, or another reason may be more vulnerable to liver damage.
3. Opioid Analgesics Are the Strongest Pain-relieving Medications
Opioid analgesics (sometimes called narcotics) are effective for many different types of pain. Usually, they are the strongest analgesics.

Opioids are chemically related to morphine, a natural substance extracted from poppies. Some opioids are extracted from other plants, and other opioids are produced in a laboratory.
Opioid analgesics are a class of medications that work by binding to specific receptors in the brain and spinal cord, known as opioid receptors, to reduce the perception of pain. These drugs can be effective for managing moderate to severe pain but also carry a risk of dependence and addiction.
3.1 The List of Opioid Analgesics Along With Some Details
- Morphine:
- Description: One of the oldest and most potent opioid analgesics.
- Uses: Commonly used for acute and chronic pain, including post-surgical pain and cancer pain.
- Forms: Available in various formulations, including oral tablets, injectable solutions, and sustained-release formulations.
- Codeine:
- Description: Generally less potent than morphine.
- Uses: Often used for mild to moderate pain. Frequently prescribed in combination with other medications, such as acetaminophen or ibuprofen.
- Forms: Available in oral formulations.
- Hydrocodone:
- Description: Semi-synthetic opioid.
- Uses: Commonly prescribed for moderate to severe pain and as an antitussive (cough suppressant).
- Forms: Often combined with acetaminophen or ibuprofen in oral formulations.
- Oxycodone:
- Description: Semi-synthetic opioid with a potency similar to morphine.
- Uses: Used for moderate to severe pain, including post-surgical and cancer pain.
- Forms: Available in immediate-release and extended-release formulations. Often combined with acetaminophen or other analgesics.
- Fentanyl:
- Description: Synthetic opioid that is highly potent.
- Uses: Used for severe pain, particularly in cancer patients. Also available in patch form for long-term pain management.
- Forms: Available in various formulations, including transdermal patches, lozenges, and injectable solutions.
- Methadone:
- Description: Synthetic opioid with unique pharmacokinetics.
- Uses: Used for chronic pain management and as part of opioid addiction treatment programs.
- Forms: Available in oral formulations.
- Hydromorphone:
- Description: Semi-synthetic opioid, more potent than morphine.
- Uses: Used for moderate to severe pain.
- Forms: Available in oral formulations and injectable solutions.
- Oxymorphone:
- Description: Semi-synthetic opioid, more potent than morphine.
- Uses: Used for moderate to severe pain.
- Forms: Available in oral formulations and injectable solutions.
- Tramadol:
- Description: Atypical opioid with both opioid and non-opioid mechanisms of action.
- Uses: Used for moderate to moderately severe pain.
- Forms: Available in oral formulations.
3.2 When to Use Opioids
- Opioids are the mainstay for treatment of the following:
Severe sudden, relatively short-lived (acute) pain, as occurs after surgery or results from burns or broken bones
Chronic pain due to cancer or another disorder that shortens lifespan (terminal disorder)
Chronic pain in people receiving hospice care
- Opioids are preferred for these disorders because opioids are so effective in controlling pain.
- Opioids may be underused in these situations because doctors
Underestimate the dose needed to be effective
Overestimate the risk of opioid side effects, such as an opioid use disorder (addiction)
- cancer or another terminal disorder or in hospice, in people with pain due to cancer or another terminal disorder or in hospice, concerns about side effects should not limit the use of opioids because side effects can usually be prevented or managed, and addiction is less of a concern.
3.3 Opioids are Usually not the First Choice
If chronic pain is not due to cancer or a terminal disorder, opioids are usually not the first choice for treatment because the side effects of long-term opioid therapy can be serious.
Opioid side effects include opioid use disorder (addiction), overdose, a dangerous slowing of breathing (respiratory depression), and death.
Thus, when chronic pain is not due to cancer or a terminal disorder, other treatments, such as nonopioid drugs and nondrug treatments, are used first. If these treatments are ineffective, doctors may consider using opioids but only when the need for pain relief and improved functioning outweighs the risks of opioids.
3.4 Opioids are not Appropriate for Everyone.
Doctors ask people questions before prescribing opioids for them. The questions are designed to determine whether people are likely to
Misuse or abuse the drug
Use them for other purposes (such as selling them or using them to fall asleep)
Have side effects from the drug
Doctors also explain what the risks and side effects of opioids are and how to take and store opioids correctly.
The dose of an opioids is increased gradually, in stages, until the pain is relieved or the opioid’s side effects cannot be tolerated. Older people and newborns, who are more sensitive to the effects of opioids, are usually given lower doses.
3.5 Opioids are most effective when taken according to a schedule, before pain becomes severe.
If an opioid alone does not provide sufficient pain relief, the dose may be increased or another drug (such as an NSAID or an adjuvant analgesic) may be added, as in the following situations:
The pain temporarily worsens.
The person needs to exercise, and movement increases the pain.
A wound dressing is about to be changed.
In people with chronic pain, increasing the dose of an opioid does not necessarily result in additional pain relief and may increase the risk of side effects.
For chronic pain, opioids are often used with nonopioid analgesics, such as nonsteroidal anti-inflammatory drugs (NSAIDs), or adjuvant analgesics, such as Gabapentin (an antiseizure drug) or Tricyclic antidepressants. Nonopioid analgesics, such as acetaminophen, are sometimes combined with opioids in a single tablet.
Doctors usually monitor the response to opioids to determine whether opioids are effectively controlling the pain and/or people are having side effects. Based on this information, doctors determine whether continuing opioid therapy is appropriate. As the pain lessens, doctors reduce the dose of the opioid gradually, and when possible, they stop the opioid and switch to or continue to take a nonopioid analgesic.
Opioids provide long-term relief for only some people who are treated with them, and usually, they only partially relieve the pain. Some people decide to stop taking opioids because the pain relief is insufficient or because they cannot tolerate the side effects.
3.6 Side Effects of Opioids
Opioids have many side effects. Side effects are more likely to occur in people with certain disorders: kidney failure, a liver disorder, chronic obstructive pulmonary disease (COPD), untreated sleep apnea, dementia, or another brain disorder.
The following commonly occur when opioids are used:
Drowsiness
Mental fuzziness or confusion
Nausea and vomiting
Constipation
Less common side effects of opioids include
Retention of urine
Involuntary contraction of muscles (called myoclonus)
Itching
A dangerous slowing of breathing
Death
Drowsiness is a common side effect of opioids. For some people who take opioids, drowsiness disappears or decreases within a few days. If people continue to feel drowsy, a different opioid can be tried because the degree of drowsiness caused by different opioids varies. Before an important event that requires alertness, people may be given a stimulant drug (such as methylphenidate or modafinil) to offset the drowsiness. For some people, drinking a caffeinated beverage helps offset the drowsiness. When feeling drowsy after taking an opioid, people should avoid driving and take extra care to prevent falls and accidents.
Confusion can also result from taking opioids, especially if people are older. Opioids increase the risk of falls in older people.
Nausea sometimes occurs in people with pain, and opioids can increase the nausea. Antiemetic drugs taken by mouth, suppository, or injection help prevent or relieve nausea. Some commonly used antiemetic drugs are metoclopramide, hydroxyzine, and prochlorperazine.
The itching caused by taking opioids may be relieved by an antihistamine such as diphenhydramine, taken by mouth or given intravenously.
Constipation often develops, especially in older people. Stimulant laxatives, such as senna, help prevent or relieve the constipation. Increasing the intake of fluids and the amount of fiber in the diet can also help. Osmotic agents such as polyethylene glycol can also be useful. These agents pull large amounts of water into the large intestine to stimulate bowel movements. Some people need enemas. When these measures are not effective, doctors may prescribe a drug (such as methylnaltrexone) that blocks only the effects of opioids in the stomach and intestine and does not lessen the pain relief.
Retention of urine can result from taking opioids, especially in men with an enlarged prostate. Trying to urinate a second time after a brief pause (double voiding) or applying gentle pressure on the lowest part of the abdomen (the area over the bladder) during urination may help. Sometimes a drug that relaxes muscles of the bladder (such as tamsulosin) is used.
For most people, nausea and itching disappear or decrease within a few days. But constipation and retention of urine usually decrease much more slowly, if at all.
3.7 Serious Side Effects of Opioids
Serious side effects can occur when people take too much of an opioid. These side effects include a dangerous slowing of breathing (respiratory depression), coma, and even death. The following adds to the risk of developing respiratory depression and of dying from respiratory arrest:
Having certain conditions (such as liver, kidney, or respiratory disorders)
Taking other drugs that cause drowsiness (such as benzodiazepines)
Drinking alcohol
Some of these side effects can be reversed with naloxone, an antidote usually given intravenously or sprayed into the nose.
For people who are at increased risk of opioid side effects (including respiratory depression), doctors may prescribe naloxone when they prescribe the opioid. Nurses and family members or caregivers should watch for serious side effects of opioids and, if such side effects occur, be ready to inject naloxone or spray it into the person’s nose. Doctors or pharmacists usually teach the person taking the opioid and family members or caregivers how to administer naloxone.
Tolerance occurs in some people who take opioids repeatedly over time. They need higher doses because their body adapts to and thus responds less well to the drug. However, for most people, the same opioid dose remains effective for a long time. Often, the need for a higher dose means that the disorder is worsening, not that tolerance is developing.
Physical dependence usually develops in people who take opioids for a long time. That is, they experience withdrawal symptoms if the drug is stopped. Withdrawal symptoms include chills, abdominal cramping, diarrhea, trouble sleeping, and a jittery feeling. When opioids are stopped after long-term use, doctors reduce the dose gradually over a period of time to minimize the development of such symptoms.
Physical dependence is not the same as addiction, which is characterized by a craving for the drug and compulsive, uncontrolled use of the drug despite the harm done to the user or other people. Most people who take opioids to control pain and have not previously had problems with drug abuse do not become addicted to opioids. Nonetheless, doctors regularly monitor people who are taking opioid analgesics for signs of addiction.
3.8 Administration of Opioids
When possible, opioids are taken by mouth (orally). When opioids are taken by mouth, the dose and time they are taken can be adjusted more easily. When they need to be taken for a long time, they may be given by mouth or through a patch placed on the skin (transdermally). Opioids are given by injection (into a muscle or vein) when pain occurs suddenly or when people cannot take them by mouth or through a skin patch.
If people who need to take opioids for a long time and are helped by an opioid taken by mouth but cannot tolerate its side effects, an opioid can be injected directly into the space around the spinal cord through a pump (intrathecally). This method gets high concentrations of the drug to the brain.
Morphine, the prototype of these drugs, can be taken by mouth or by injection. Morphine comes in sustained-, controlled-, and immediate-release forms that are taken by mouth.
The immediate-release form of morphine provides short-lived relief (about 4 hours) and is usually used to treat acute pain.
The controlled- and sustained-release forms provide relief for 8 to 24 hours. These forms have been widely used to treat chronic pain when nonopioid analgesics do not provide sufficient pain relief. However, if pain is not related to cancer, experts recommend limiting the use of these long-acting (controlled- and sustained-release) opioids.
Rapid-acting opioids (lozenges or dissolvable tablets) are placed under the tongue (sublingual) or between the gums and cheek (buccal). There, they are allowed to dissolve and are absorbed through the mucous membrane that lines the cheek or that lies under the tongue. These forms should not be swallowed. They provide relief very rapidly. Because they work rapidly, risk of side effects may be greater. They are used for breakthrough pain in people with cancer. Breakthrough pain is a brief, often severe flare-up of pain that may occur when regularly scheduled treatment does not control pain.
In injected forms, 3 times less morphine is required than in the immediate-release oral form because when morphine is taken by mouth, much of the drug is chemically altered (metabolized) by the liver before it reaches the bloodstream. Usually, the route used does not change the drug’s effects, even though different routes use different amounts of morphine.
Pain relief with injected forms is quicker than that with oral forms, but relief does not last as long.
Morphine may be injected into a vein (intravenously), into a muscle (intramuscularly), or under the skin (subcutaneously).
Intravenously: Pain relief is almost immediate but does not last very long.
Intramuscularly: Pain relief is less rapid but lasts somewhat longer. Intramuscular injections are painful, and pain relief is less predictable, so this route is not used often.
Subcutaneously: Pain relief is the least rapid but lasts the longest.
Injections can be given every few hours, but repeated injections can become annoying. Alternatively, a catheter can be inserted in a vein or under the skin and connected to a continuous-infusion pump, which supplies morphine continuously. The continuous infusion can be supplemented with extra doses when needed. Sometimes a device that enables a person to release the drug by pressing a button is used. However, the doctor determines how much of the drug is released and how often it can be released. This technique is called patient-controlled analgesia. Usually, continuous infusion is used for people who are hospitalized and who have severe pain that occurs after surgery or that is due to a serious disorder such as cancer or a sickle cell crisis.
3.9 Problems With the use of Opioids
Opioids are now the leading cause of accidental death and fatal drug overdose in the United States. Problems with using opioids include opioid misuse, diversion, and abuse.
Opioid misuse may be intentional or unintentional. It includes any use that differs from what is prescribed.
Diversion involves selling or giving a prescribed drug to others.
Abuse refers to recreational use of the drug. That is, the drugs are taken for the feelings of pleasure or sensations they produce, rather than to treat pain or another medical condition.
Up to one third of people taking opioids for a long time to treat chronic pain may misuse them.
Opioid use disorder is the preferred term for what previously was called opioid addiction. It refers to compulsive use of opioids despite having problems caused by taking them. Also, people who have this disorder may require higher and higher doses to achieve the same effects and may experience withdrawal symptoms when they stop taking the opioid. They may try to stop taking opioids or reduce the amount they are taking but cannot. Taking high doses of opioids for a long time increases the risk of developing opioid use disorder.
Before prescribing opioids, doctors should evaluate people for risk factors for problems with taking opioids. Risk factors include
Problems with alcohol or drugs in the past
Family members who have had problems with alcohol or drugs
Mental health disorders such as poorly controlled anxiety, depression, or bipolar disorder
Use of other drugs that affect brain function
Age under 45 years
When the opioid is first prescribed, doctors explain the risks of opioids and the measures used to ensure that the drug is used safely. If problems occur, people are also told that they may be referred to a substance use specialist.
Doctors closely monitor all people who are treated with opioids to make sure opioid therapy is used safely. For example, they may test for other recreational drugs. Doctors also monitor interconnected state databases that track opioid prescriptions to check whether people are getting opioid prescriptions at more than one pharmacy. To prevent misuse, doctors typically restrict the person to a single pharmacy for filling opioid prescription.

3.10 What is the Precaution of Taking Opioid Analgesics ?
Taking opioid analgesics requires careful consideration and adherence to precautions to minimize the risk of adverse effects and complications. Here are some general precautions associated with the use of opioid analgesics:
- Prescription and Monitoring:
- Opioid analgesics should only be taken under the supervision and prescription of a qualified healthcare professional.
- Regular monitoring and follow-up appointments are necessary to assess the effectiveness of the treatment and to manage potential side effects.
- Individualized Treatment Plans:
- The choice of opioid, dosage, and duration of treatment should be individualized based on the patient’s specific medical condition, pain intensity, and response to the medication.
- Risk Assessment:
- Healthcare providers should conduct a thorough assessment of the patient’s medical history, including any history of substance abuse, mental health conditions, and respiratory issues, to determine the suitability of opioid therapy.
- Tolerance and Dependence:
- Opioids can lead to the development of tolerance, where higher doses are needed over time to achieve the same level of pain relief. Dependence can also occur, leading to withdrawal symptoms when the medication is discontinued. Patients should be monitored for these phenomena.
- Avoiding Alcohol and Sedatives:
- Combining opioids with alcohol or sedative medications can enhance sedation and respiratory depression, increasing the risk of overdose. Patients should avoid alcohol and inform their healthcare provider about all medications they are taking.
- Respiratory Function Monitoring:
- Opioids can depress respiratory function, especially at higher doses. Patients with pre-existing respiratory conditions, such as asthma or chronic obstructive pulmonary disease (COPD), require close monitoring.
- Constipation Management:
- Opioids commonly cause constipation. Patients should maintain adequate fluid intake, dietary fiber, and, if necessary, use stool softeners or laxatives as recommended by their healthcare provider.
- Driving and Operating Machinery:
- Opioids can cause drowsiness and impair cognitive function. Patients should be cautious about driving or operating heavy machinery while taking these medications.
- Pregnancy and Breastfeeding:
- Pregnant or breastfeeding individuals should consult their healthcare provider before using opioids, as these medications can pass through the placenta or breast milk and affect the baby.
- Proper Storage:
- Opioid medications should be stored securely to prevent misuse or accidental ingestion by others, especially in households with children.
It’s crucial for patients to communicate openly with their healthcare provider about their pain levels, any side effects, and any concerns they may have regarding opioid therapy. Patients should never self-adjust their opioid dosage or abruptly stop taking the medication without consulting their healthcare provider, as this can lead to withdrawal symptoms and other complications.
4. Adjuvant Analgesics
Increasingly, an adjuvant analgesic is the first and only drug used to treat pain due to nerve damage (neuropathic pain) and conditions such as fibromyalgia.
The adjuvant analgesics most commonly used for pain are
Antidepressants (such as amitriptyline, bupropion, desipramine, duloxetine, nortriptyline, and venlafaxine)
Antiseizure drugs (such as gabapentin and pregabalin)
Oral and topical local anesthetics
4.1 Antidepressants
Antidepressants can often relieve pain in people even when they do not have depression. Tricyclic antidepressants (such as amitriptyline, nortriptyline, and desipramine) may be more effective for this purpose than other antidepressants, but newer antidepressants, such as selective serotonin reuptake inhibitors (SSRIs) and norepinephrine reuptake inhibitors (SNRIs, including duloxetine, venlafaxine, and milnacipran) may have fewer of the side effects that limit how much of the drug can be taken.
Tricyclic antidepressants are effective for neuropathic pain, headaches, fibromyalgia, and visceral (organ) hypersensitivity syndromes (such as chronic abdominal or pelvic pain). The doses of tricyclic antidepressants used to treat pain are usually too low to treat depression or anxiety. Thus, if tricyclic antidepressants are used to treat pain, additional drugs are usually needed to treat depression or anxiety if present.
Duloxetine appears to be effective for neuropathic pain due to diabetes (called diabetic neuropathy), fibromyalgia, chronic low back pain, chronic musculoskeletal pain, and nerve pain due to chemotherapy. The doses of duloxetine used to treat pain are also adequate to treat depression or anxiety if present. Venlafaxine has similar effects. Milnacipran is effective for fibromyalgia.
People may respond to one antidepressant and not to others.
4.2 Antiseizure drugs
Antiseizure drugs may be used to relieve neuropathic pain. Gabapentin and pregabalin are most commonly used, but many others, including carbamazepine, clonazepam, lacosamide, lamotrigine, oxcarbazepine, phenytoin, topiramate, and zonisamide, help relieve pain in some people.
Gabapentin can be used to treat the pain that can result from shingles (postherpetic neuralgia) and many other types of neuropathic pain.
Pregabalin can be used to relieve pain caused by fibromyalgia or nerve damage due to diabetes (diabetic neuropathy), postherpetic neuralgia, or neuropathic pain due to a problem in the brain or spinal cord.
Antiseizure drugs, such as topiramate, can prevent migraine headaches.
4.3 Anesthetics
A local anesthetic, such as lidocaine, may be injected into the skin to control pain due to an injury or even neuropathic pain. Local anesthetics can also be injected around nerves to block pain—a procedure called a nerve block. For example, a sympathetic nerve block involves injecting a local anesthetic around a group of nerves near the spine—in the neck for pain in the upper body or in the lower back for pain in the lower body.
Topical anesthetics, such as lidocaine applied as a lotion, an ointment, or a skin patch, can be used to control pain due to some conditions.
Mexiletine, used to treat abnormal heart rhythms, is sometimes used to treat neuropathic pain.
These anesthetics are usually used for a short period of time. For example, rinsing with small amounts of an anesthetic mouthwash a few times a day can relieve pain due to mouth sores. However, some people with chronic pain benefit from using topical anesthetics for a long time. For example, a lidocaine patch or gel can help relieve postherpetic neuralgia.
Anesthetics are substances or drugs that induce a reversible loss of sensation or consciousness, allowing medical procedures to be performed without causing pain or discomfort. There are different types of anesthetics, and they can be categorized based on their primary effects.
The main types of anesthetics are:
- Local Anesthetics:
- Description: Local anesthetics block nerve signals in a specific area of the body, leading to temporary loss of sensation. They are often used for minor surgical procedures or dental work.
- Examples: Lidocaine, bupivacaine, procaine.
- Regional Anesthetics:
- Description: Regional anesthetics target a larger part of the body, such as an entire limb, by blocking nerve signals in a specific region. These can include spinal and epidural anesthesia.
- Examples: Bupivacaine, ropivacaine.
- General Anesthetics:
- Description: General anesthetics induce a state of unconsciousness, rendering the patient completely unaware and unresponsive to pain during surgery or other medical procedures.
- Examples: Inhalation agents like desflurane, sevoflurane, and intravenous agents like propofol.
- Intravenous Anesthetics:
- Description: Administered through the bloodstream, these anesthetics induce sedation, amnesia, and loss of consciousness. They are commonly used in combination with inhaled anesthetics during general anesthesia.
- Examples: Propofol, etomidate, thiopental.
- Inhalation Anesthetics:
- Description: These anesthetics are administered by inhaling a gas or vapor. They play a key role in maintaining general anesthesia during surgery.
- Examples: Desflurane, sevoflurane, nitrous oxide.
- Adjunct Anesthetics:
- Description: These are medications used in combination with other anesthetics to enhance their effects, manage side effects, or provide additional analgesia.
- Examples: Opioids (e.g., fentanyl), muscle relaxants (e.g., rocuronium).
4.4 Other drugs
Corticosteroids, such as prednisone and dexamethasone, can be taken by mouth if severe pain is caused by inflammation (as occurs in gout).
Some evidence suggests that baclofen (a muscle relaxant) can help relieve neuropathic pain due to trigeminal neuralgia.
Pamidronate (used to treat certain bone disorders) can help relieve neuropathic pain due to complex regional pain syndrome.
Low doses of ketamine (an anesthetic) are sometimes given intravenously in a hospital to people who have complex regional pain syndrome when other treatments are ineffective.
Tizanidine (a muscle relaxant), taken by mouth, and clonidine (used to treat high blood pressure), taken by mouth or applied to the skin as a patch, can help relieve neuropathic pain or prevent migraines.
High-strength capsaicin (a substance found in hot peppers), given in a patch, helps relieve neuropathic pain due to postherpetic neuralgia. A low-strength capsaicin cream may also help reduce the pain caused by postherpetic neuralgia and by other disorders such as osteoarthritis. The cream is most often used by people with localized pain due to arthritis. This cream must be applied several times a day.
Pain Medications, Pain Relief, and Pain Management
")

")




?")