Anticonvulsant medications are prescribed to manage and prevent seizures. Anticonvulsant medications, also known as antiepileptic drugs (AEDs) or antiseizure drugs, are a class of pharmaceuticals used to treat and manage epileptic seizures. Epilepsy is a neurological disorder characterized by recurrent, unprovoked seizures, which are caused by abnormal electrical activity in the brain. Anticonvulsant medications work by stabilizing the electrical activity in the brain, preventing or reducing the occurrence of seizures.

These medications are not only used for epilepsy but may also be prescribed for other conditions involving abnormal electrical activity in the brain, such as certain mood disorders, neuropathic pain, and migraines.
Dosages and specific instructions can vary depending on the individual and their medical condition. Here are some common anticonvulsant medications:
- Phenytoin (Dilantin):
- Dosage: The initial dose is usually 100 mg three times a day. Maintenance doses are typically 200-300 mg per day.
- Administration: It can be taken with or without food.
- Carbamazepine (Tegretol):
- Dosage: The starting dose is often 200 mg twice a day, with a gradual increase.
- Administration: It can be taken with or without food.
- Valproic Acid (Depakote):
- Dosage: Initial doses are often 250 mg twice a day, with adjustments based on response and tolerance.
- Administration: It can be taken with food to reduce stomach upset.
- Lamotrigine (Lamictal):
- Dosage: The initial dose is usually low, with a gradual increase to avoid skin rash. Maintenance doses vary.
- Administration: It can be taken with or without food.
- Levetiracetam (Keppra):
- Dosage: The initial dose is often 500 mg twice a day, with adjustments based on response.
- Administration: It can be taken with or without food.
- Gabapentin (Neurontin):

- Dosage: Starting doses are typically low and gradually increased.
- Administration: It can be taken with or without food.
- Topiramate (Topamax):
- Dosage: Initial doses are often low, with gradual titration.
- Administration: It can be taken with or without food.
- Oxcarbazepine (Trileptal):
- Dosage: Initial doses are based on body weight, and adjustments are made gradually.
- Administration: It can be taken with or without food.
- Pregabalin (Lyrica):
- Dosage: It is usually started at a low dose and adjusted based on response.
- Administration: It can be taken with or without food.
- Zonisamide (Zonegran):
- Dosage: Usually started at 100 mg per day.
- Administration: With or without food.
- Clonazepam (Klonopin):
- Dosage: Low initial doses.
- Administration: With or without food.
- Clobazam (Onfi):
- Dosage: Variable, based on age and weight.
- Administration: With or without food.
- Ethosuximide (Zarontin):
- Dosage: Variable based on age.
- Administration: With or without food.
- Lacosamide (Vimpat):
- Dosage: Initiated at 50 mg twice a day.
- Administration: With or without food.
- Perampanel (Fycompa):
- Dosage: Typically initiated at 2 mg per day.
- Administration: With or without food.
- Rufinamide (Banzel):
- Dosage: Initiated at 400-800 mg per day.
- Administration: With or without food.
- Tiagabine (Gabitril):
- Dosage: Variable, usually initiated at low doses.
- Administration: With or without food.
- Vigabatrin (Sabril):
- Dosage: Variable, based on weight.
- Administration: With or without food.
- Acetazolamide (Diamox):
- Dosage: Variable, depending on the condition.
- Administration: With or without food.
- Fosphenytoin (Cerebyx):
- Dosage: IV form, administered in hospital settings.
- Primidone (Mysoline):
- Dosage: Gradual titration.
- Administration: With or without food.
- Stiripentol (Diacomit):
- Dosage: Based on weight.
- Administration: With or without food.
- Diazepam (Valium):
- Dosage: Variable, depending on the situation.
- Administration: As prescribed.
- Methsuximide (Celontin):
- Dosage: Variable.
- Administration: With or without food.
- Nicardipine (Cardene):
- Dosage: IV form, administered in hospital settings.
- Oxazepam (Serax):
- Dosage: Variable.
- Administration: As prescribed.
- Piracetam (Nootropil):
- Dosage: Variable.
- Administration: With or without food.
- Sodium Valproate (Depacon):
- Dosage: Variable.
- Administration: With or without food.
- Vigabatrin (Sabril):
- Dosage: Variable, based on weight.
- Administration: With or without food.
- Zinc Sulfate:
- Dosage: Variable.
- Administration: With or without food.
How Does Anticonvulsant Medications Work ?
Anticonvulsant medications work by stabilizing the electrical activity in the brain, specifically by modulating neurotransmission and ion channel function. Epileptic seizures are caused by abnormal and excessive electrical discharges in the brain, disrupting normal communication between neurons. Anticonvulsants aim to prevent or reduce these abnormal electrical activities, thereby controlling seizures. The exact mechanisms of action can vary among different anticonvulsant drugs, but some common ways they work include:
- Sodium Channel Modulation:
- Many anticonvulsants, such as phenytoin and carbamazepine, target voltage-gated sodium channels. These channels play a crucial role in the initiation and propagation of action potentials in neurons. By stabilizing sodium channels, anticonvulsants help regulate the flow of sodium ions and prevent excessive neuronal firing.
- Calcium Channel Modulation:
- Some anticonvulsants, like valproic acid, work by modulating voltage-gated calcium channels. These channels are involved in neurotransmitter release and maintaining neuronal excitability. By regulating calcium influx, anticonvulsants can help stabilize neuronal activity.
- GABAergic Enhancement:
- GABA (gamma-aminobutyric acid) is an inhibitory neurotransmitter that helps regulate neuronal excitability. Certain anticonvulsants, such as benzodiazepines (e.g., clonazepam), enhance the effects of GABA by binding to specific receptors. This leads to increased inhibitory signaling and a reduction in abnormal neuronal activity.
- Glutamate Receptor Modulation:
- Glutamate is an excitatory neurotransmitter that plays a role in neuronal communication. Anticonvulsants like lamotrigine and topiramate modulate glutamate receptors, reducing the excessive excitatory signaling associated with seizures.
- Potassium Channel Modulation:
- Some anticonvulsants, including retigabine, affect voltage-gated potassium channels. Modulating these channels helps stabilize the resting membrane potential of neurons, making it less likely for them to generate abnormal electrical discharges.
- Neuronal Stabilization:
- Anticonvulsants aim to stabilize the overall balance between excitatory and inhibitory neurotransmission in the brain. By doing so, they reduce the likelihood of abnormal synchronized neuronal firing that can lead to seizures.
It’s important to note that the specific mechanism of action can vary widely among different anticonvulsant medications, and some drugs may have multiple targets. Additionally, individual responses to these medications may vary, and the choice of anticonvulsant depends on factors such as the type of seizures, the patient’s age, and overall health.
What Are Side Effects of Anticonvulsant Medications ?
Anticonvulsant medications, like any drugs, can have side effects. It’s important to note that not everyone will experience these side effects, and the severity can vary. Additionally, the specific side effects may depend on the individual medication. Below are some common side effects associated with anticonvulsant medications:
- Drowsiness or Fatigue:
- Many anticonvulsants can cause drowsiness or fatigue, especially when treatment is initiated or the dosage is increased.
- Dizziness or Lightheadedness:
- Some people may experience dizziness or lightheadedness, particularly when standing up quickly.
- Nausea and Vomiting:
- Gastrointestinal symptoms such as nausea and vomiting can occur with certain anticonvulsants.
- Cognitive Impairment:
- Some individuals may experience difficulty concentrating, memory problems, or other cognitive impairments.
- Mood Changes:
- Anticonvulsants can sometimes affect mood, leading to changes such as irritability, depression, or anxiety.
- Weight Changes:
- Weight gain or loss can be a side effect of certain anticonvulsant medications.
- Skin Rash:
- Some anticonvulsants, such as lamotrigine, are associated with an increased risk of skin rash, which can be severe.
- Hair Loss:
- Hair loss or changes in hair texture can occur with certain anticonvulsants.
- Liver Problems:
- Some anticonvulsants may affect liver function, leading to potential liver problems.
- Bone Health Issues:
- Long-term use of certain anticonvulsants, especially in high doses, may affect bone health and increase the risk of fractures.
- Blood Disorders:
- Rarely, anticonvulsants may cause blood-related disorders, such as decreased platelet count or white blood cell count.
- Teratogenic Effects:
- Some anticonvulsants, if taken during pregnancy, may increase the risk of birth defects. It’s crucial for women of childbearing age to discuss the potential risks and benefits with their healthcare provider.
- Kidney Function:
- Certain anticonvulsants may impact kidney function in some individuals.
- Hyponatremia:
- Some anticonvulsants can cause low sodium levels in the blood, leading to symptoms like nausea, headache, confusion, and seizures.
General Points
- Brand vs. generic. Every medicine has a brand and a generic name. The generic usually is cheaper, sometimes by quite a lot. For medicines introduced in recent years, patent (or “market exclusivity”) protection may block the sale of generic versions. A generic medicine usually works well, but it may not generate the same blood levels as does the brand name or an alternative generic medicine. Therefore, with changes of pill manufacturers, the blood levels can change. This may produce breakthrough seizures or side effects. The most important concern when taking generic drugs is to be sure the tablets are made by the same manufacturer for each refill. Switching from one generic manufacturer to another could result in different amount of active drug in each pill. The current author supports the right of the patient and doctor to know about medication substitution and consider whether generic substitution is safe.
- Starting schedule: Many AEDs have to be started slowly to minimize side effects, event though this delays helping the seizures. The titration (starting) schedules are those of the author, and may be slower than is the schedule recommended in the package insert. Dosages are all for adults. Children are treated on the basis of their weight (mg per kg dosing basis).
- Monotherapy: Some AEDs have approval for monotherapy (to be used alone) and others only as adjunctive (add-on) therapy to another AED. This reflects what testing evidence has been presented to the FDA – not all AEDs have gone through the required two clinical studies to show effectiveness in monotherapy. AEDs not proven effective in monotherapy still probably work well as single medications and are used that way by epilepsy doctors on a case-by-case basis where the benefit seems to exceed the risk.
- Blood levels: Target blood levels are broad guides to clinical use. Actual blood levels differ for different laboratories. The desirable level depends upon the type and number of seizures, side effects, taking one vs. multiple drugs and other clinical factors.
- Side effects: Side effects listed below are a brief compilation of the most common and most worrisome, not a full list. Every seizure medicine can sometimes cause side effects of fatigue, dizziness, unsteadiness, blurry vision, stomach upset, headaches, and reduced resistance to colds, memory and thinking problems. Weight gain tends to occur with valproic acid (Depakote), gabapentin (Neurontin), pregabalin (Lyrica) and carbamazepine (Tegretol, Carbatrol). Weight loss tends to occur with topiramate (Topamax), zonisamide (Zonegran) and felbamate (Felbatol). These are not mentioned separately in each section, unless they are especially common with the medicine. Detailed information is provided by the pharmacy as a package insert for new prescriptions and refills.
- Effects on internal organs: All seizure medicines can cause problems with blood counts (white cells, red cells and platelets), or liver or other internal organs, so doctors usually order blood tests to screen for these problems. Blood can be tested when starting a medicine to get a baseline, after a few months on the drug, every few months to yearly thereafter, then at individually determined times. The package insert often has recommendations, but there are no universal rules about when to test blood. All seizure medicines can produce either mild or severe allergic reactions. One, called the hypersensitivity syndrome, produces fever, rash, fluid accumulation, swollen lymph nodes, possible liver injury and confusion
- Suicide warning: The US FDA has required a suicide warning on all seizure medications as a general class. All people taking them should be aware of and report any serious depression or suicidal thinking to their doctor, but the actual risk for suicide due to AEDs is quite low.
- Mechanism: Mechanisms of action in the brain for antiepileptic drugs are described in simple form: most AEDs have multiple mechanisms of action to block seizures.
- Not a cure: Although AEDs are called “antiepileptic,” they do not cure epilepsy, but just suppress seizures while the medications are in the body.
Antiepileptic Drugs (AEDs), alphabetically
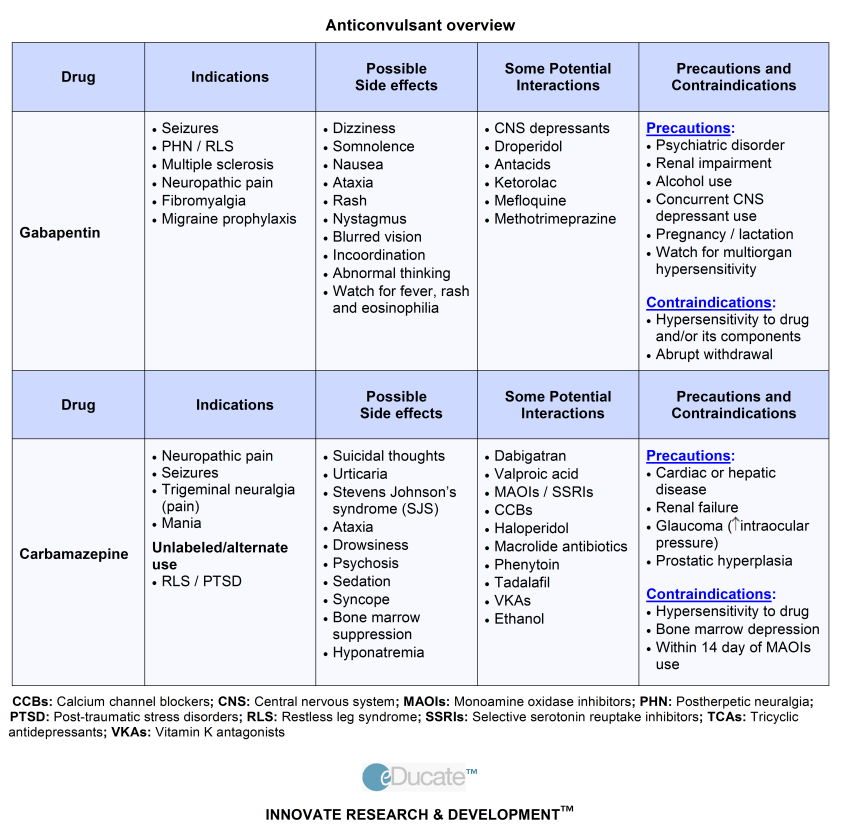
carbamazepine (Tegretol, Carbatrol): A favorite partial seizure medicine in the developed world. Carbamazepine affects sodium channels, and inhibits rapid firing of brain cells. Long-acting forms such as Carbatrol or Tegretol-XR can be given once a day. Potential side effects include GI upset, weight gain, blurred vision, low blood counts, low blood sodium (hyponatremia). Carbamazepine causes a rash rate of a few percent, sometimes even the dangerous rash called Stevens-Johnson syndrome. People of Asian descent with HLA-B*1502 antigen are more at risk. Typical adult dose is 400 mg tid. I start my patients with 200 mg bid and each week, and increase by 200 mg daily to about 400 mg three times a day. See information on carbamazepine and information about carbamazepine extended release.
clonazepam (Klonopin): Clonazepam is a member of the drug class known as benzodiazepines, to which diazepam (Valium), lorazepam (Ativan), clorazepate (Tranxene), alprazolam (Xanax) also belong. Benzodiazepines are used as anti-seizure drugs, sedatives, tranquilizers and muscle relaxants. Benzodiazepines increase the effectiveness of GABA, the brain’s main inhibitory neurotransmitter. Clonazepam is more long-acting against seizures than are diazepam or lorazepam. Side effects of clonazepam include sedation, thinking/memory impairment, mood changes, addiction. More so than most, its effects wear off over time. A typical adult dose is 0.5-1.0 mg three times a day. I usually start my patients with 0.5 mg at night, and if they are not too sleepy the next day, increase to 0.5 mg twice a day. A week later, if seizures persist, I will increase to 0.5 mg three times a day. See information on clonazepam.
gabapentin (Neurontin): Gabapentin has the reputation of being a safe but not particularly powerful AED. The effectiveness criticism probably is because it is often prescribed at too low a dose. The drug probably works by influencing transport of GABA and effects on calcium channels. It has no drug interactions, is not metabolized in the liver and it does not bind to blood proteins. Side effects are unsteadiness, weight gain, fatigue, dizziness. Typical adult dose is 300-600 mg three times a, but doses can be up to 1200 mg three times a day. I often start at 300 mg per day, sometimes in one dose or with 100 mg pills, and increase over a month or two to the full dose. Gabapentin often is used also for chronic pains of certain types. See information on gabapentin.
lacosamide (Vimpat): Lacosamide is a new (2009) antiepileptic drug , for partial and secondarily generalized seizures. It is chemically related to the amino acid, serine. Vimpat blocks sodium channels (but in a different way from other seizure medicines), and this block reduces brain excitability. Side effects include dizziness, headache, nausea or vomiting, double vision, fatigue, memory or mood problems. Vimpat may affect the internal organs, blood counts or heart rhythm, but these potentially serious side effects are infrequent. The recommended starting dose is 50 mg twice daily, increased each week by an extra 100 mg, to the recommended maintenance dosage of 100-200 mg twice a day. See information on lacosamide.
lamotrigine (Lamictal): A broad-spectrum alternative to VPA, with a better side effect profile. However, LTG may not be as effective for myoclonic seizures. Lamotrigine works by several mechanisms including blocking release of glutamate, the brain’s main excitatory neurotransmitter. It has the usual side effects of dizziness and fatigue, usually mild cognitive (thinking) impairment. Severe medical side effects are unusual. The practical side effect issue is rash, occurring in several percent of people who take it, especially if the dose is increased too fast. Therefore, it takes a couple of months to get up to the typical adult dose of 200 mg twice a day. I usually start my patients at low doses, adding one 25 mg pill daily each week on a two-times-a-day schedule until taking 100 mg twice a day. If there is no rash at that time, one is unlikely. I then switch my patients to 100 mg pills and increase to 200 mg twice a day over the next few weeks. This is slower than the package insert suggested starting dose, however, a slow starting dose is especially important if the patient also takes valproic acid (Depakote), to reduce risk for rash. Lamotrigine is also used for mood stabilization. See information on lamotrigine.
levetiracetam (Keppra): Levetiracetam is one of the more used medicines in seizure clinics because it probably is effective for a broad-spectrum of seizures types, has a relatively low incidence of causing thinking/memory problems, and can be started at 500 mg twice a day, which is an effective dose. It has no drug interactions, is not metabolized in the liver and it does not bind to blood proteins. The most common side effects are dizziness, fatigue, insomnia, but the more troublesome problem can be irritability and mood changes. This may occur to some degree in up to a third of those taking the medicine. A typical adult dose is 500 – 1500 mg twice a day. I usually start my patients with 250 mg twice a day and increase the next week to 500 mg twice a day, then the next week to 1000 mg in the am plus 500 mg in the pm, then the week after to 1000 mg twice a day. This is slower than the package insert suggested starting dose. See information on levetiracetam.
lorazepam (Ativan): Lorazepam is similar to clonazepam in dosage and action, but it is not as long-acting. It is usually used as a ‘rescue medication’ for patients who frequently have clusters of seizures. It works reasonably quickly when taken orally and anti-seizure effect lasts for 2-6 hours. Typical adult dose is 0.5-2.0 mg orally or as needed. A lorazepam concentrate, 2 mg per ml, can be taken as 1 ml liquid under the tongue in urgent situations. See information on lorazepam.
oxcarbazepine (Trileptal): Slightly different from carbamazepine, it is at least as effective, and may have fewer side effects, except for more risk for low blood sodium (hyponatremia). It is more expensive than generic carbamazepine. A typical adult dose is 600 mg twice a day. I start my patients with 150 mg twice a day, and increase by 150 mg daily each week. This is slower than the package insert suggested starting dose. An immediate switch from carbamazepine to full-dose oxcarbazepine is possible in some cases. See information on oxcarbazepine.
phenobarbital (Luminal): The old-timer: very inexpensive and effective in a single daily dose. Phenobarbital increases the effect of GABA, the main inhibitory neurotransmitter in the brain. Watch for sedation, thinking/memory problems and depression. Phenobarbital can cause long-term bone problems. Phenobarbital is mildly addictive and requires slow withdrawal. During pregnancy, there is a significant rate of birth defects. Typical adult dose is around 100 mg per day. I start my patients with 30 mg pills, 2 or 3 at bedtime, to allow for future dosage flexibility. The target serum level is 10-40 mcg per ml. See information on phenobarbital.
phenytoin (Dilantin): The most used AED by general physicians in the US, less so by epilepsy doctors, because of the side effects. Phenytoin alters brain cell sodium channels, which has the effect of limiting rapid firing of the brain cells. It is inexpensive. Common side effects are unsteadiness and moderate cognitive problems. There are long-term potential cosmetic (body/face hair growth, skin problems), and bone problems (osteoporosis). Phenytoin causes a rash rate of a few percent, sometimes even the dangerous rash called Stevens-Johnson syndrome. Typical adult dose is 300-400 mg per day, usually with 100 mg pills. Phenytoin can be started quickly in an emergency with intravenous administration, or a large dose of capsules if an immediate effect is required. Small changes in phenytoin dose can cause large changes in serum drug levels, so the blood levels can be hard to regulate. The target serum level is 10-20 mcg per ml. See information on phenytoin.
pregabalin (Lyrica): A relative of gabapentin, it may be better, and can be given twice a day. Some believe that it is more effective against seizures than is gabapentin. Pregabalin has no drug interactions, no liver metabolism, no protein binding, and similar side effects to gabapentin. Typical adult dose is 150 – 600 mg bid. I usually start my patients with 50 mg daily, adding 50 mg each week on a twice a day basis until taking 300 – 600 mg per day. This is slower than the package insert suggested starting dose, but avoid sedation. Pregabalin often is used also for chronic pains of certain types. See information on pregabalin.
rufinamide (Banzel, Inovelon in Europe): Banzel is approved for add-on treatment of children age 4 and older and adults with Lennox Gastaut Syndrome. This syndrome can include seizure types such as atonic (drop) seizures, tonic (stiffening) seizures, myoclonic (brief jerking) seizures, or staring (absence) seizures, as well as partial seizures. Banzel works on sodium channels in brain cells, in a way to make them less excitable. Common side effects include headache, dizziness, fatigue and sleepiness, double vision and tremor (trembling). People who have the “short QT syndrome,” a rare heart rhythm irregularity, should not take Banzel. The drug comes as 200 and 400 mg tablets. Children will usually be started at doses of approximately 10 mg/kg/day administered in two equally divided doses. Dosing can increase by adding additional 10 mg/kg amounts every two days, until the child is taking 45 mg/kg/day or a maximum of 3200 mg/day, divided into two doses each day. See information on rufinamide.
topiramate (Topamax): A good broad-spectrum AED (i.e., treats all types of seizures). Topiramate has several mechanisms, including blocking the enzyme carbonic anhydrase, which affects the acidity of brain tissue. More acidity (to a point) suppresses seizures. Side effects include thinking and memory problems in about 1/3rd, renal stones in 1-2%, rare cases of glaucoma (increased eye pressure) and weight loss. Typical adult dose is 150-200 mg twice a day. I usually start my patients with one 25 mg pill daily, adding another pill each week on a two-times-a-day schedule until taking 100 mg twice a day. If there are no significant side effects, I then switch my patients to 100 mg pills and increase to 200 mg twice a day over the next few weeks. Topiramate also is used for migraine headache prevention. See information on topiramate.
valproic acid (Depakote): This is the standard broad-spectrum AED (treats all types of seizures) and no other AED is more effective for generalized seizure types. VPA has effects on GABA (at least in very high doses), and a neurotransmitter called NPY to block seizures, and maybe also on calcium channels. VPA has significant side effects: weight gain, tremor, hair loss, GI upset, blood count decreases, hepatic or pancreatic injury, bone weakness over time (osteoporosis), birth defects in up to 10% (folic acid can help to prevent them). Typical adult dose is 250 mg – 500 mg three times a day, but dose can be higher. An extended release form can be taken once a day. See information on valproic acid.
vigabatrin (Sabril): At time of this writing, vigabatrin is approved in the US, but official package insert information has not become available. Vigabatrin is a “designer drug,” made to block metabolism of GABA, the brain’s main inhibitory neurotransmitter. Sabril has been used for over a decade in many countries, and it is effective for partial seizures, with or without secondary generalization. It also may be very effective for infantile spasms, a serious type of seizures in young children. Release in the US was delayed because the drug is toxic to the retina of the eye in up to 30% of people who take it long-term. This toxicity can result in permanent loss of peripheral vision. Regular vision testing is recommended for all people on this drug. A typical regimen begins with 500 mg twice a day, and can increase over a month or two to 1500 mg twice a day. See information on vigabatrin.
zonisamide (Zonegran): Zonisamide is rather similar in its coverage and side effects to topiramate, except glaucoma is not usually listed. Some find less cognitive impairment than with topiramate but this is individual and dose-dependent. Typical adult dose is 100-300 mg twice a day. I usually start my patients with one 25 mg pill daily, adding 25 mg each week on a two-times-a-day schedule until taking 100 mg twice a day. If there are no significant side effects, I then switch my patients to 100 mg pills and increase to 200 mg twice a day over the next few weeks. See information on zonisamide.
Others:
- acetazolamide (Diamox),
- diazepam rectal gel (Diastat),
- ethosuximide (Zarontin),
- felbamate (Felbatol),
- primidone (Mysoline),
- tiagabine (Gabitril)
Pain Medications, Pain Relief, and Pain Management
")

")



