Some people with cancer are more afraid of the pain than of the cancer. But most pain from cancer or cancer treatments can be controlled. As with all pain, it’s best to start managing cancer pain early. It might take a while to find the best approach. Pain is a highly prevalent symptom in patients with cancer. Despite therapeutic advances and well-accepted treatment guidelines, a percentage of patients with pain are under-treated.
Currently, it has been recognized that several barriers in pain management still exist and, in addition, there are new challenges surrounding complex subtypes of pain, such as breakthrough and neuropathic pain, requiring further reviews and recommendations. This is an update of the guide our society previously published and represents the continued commitment of SEOM to move forward and improve supportive care of cancer patients.
One special concern in managing cancer pain is “breakthrough pain.” This is pain that comes on quickly and can take you by surprise. It can be very upsetting. After one attack, many people worry it will happen again. This is another reason to talk with your doctor about having a pain management plan in place.
Cancer, cancer treatment, or diagnostic tests may cause you pain.
Pain is one of the most common symptoms in cancer patients. Pain can be caused by cancer, cancer treatment, or a combination of factors. Tumors, surgery, intravenous chemotherapy, radiation therapy, targeted therapy, supportive care therapies such as bisphosphonates, and diagnostic procedures may cause you pain.
Younger patients are more likely to have cancer pain and pain flares than older patients. Patients with advanced cancer have more severe pain, and many cancer survivors have pain that continues after cancer treatment ends.
This summary is about ways to control cancer pain in adults.
Pain can be managed before, during, and after tests and procedures.
Some tests and procedures are painful. It helps to start pain control before a procedure begins. Some drugs may be used to help you feel calm or fall asleep. Therapies such as imagery or relaxation can also help control pain and anxiety related to treatment. Knowing what will happen during the procedure and having a family member or friend stay with you may also help lower anxiety.
Different cancer treatments may cause specific types of pain.
Patients may have different types of pain depending on the treatments they receive, including:
- Postoperative pain.
- Spasms, pain, stinging, and itching caused by intravenous chemotherapy.
- Mucositis (sores or inflammation in the mouth or other parts of the digestive system) caused by chemotherapy or targeted therapy.
- Ostealgia (bone pain) caused by treatment with filgrastim or pegfilgrastim, which are granulocyte colony-stimulating factors that help the body make more white blood cells.
- Peripheral neuropathy (pain, numbness, tingling, swelling, or muscle weakness in hands or feet) caused by chemotherapy or targeted therapy.
- Pain in joints and muscles throughout the body caused by paclitaxel or aromatase inhibitor therapy.
- Osteonecrosis of the jaw caused by bisphosphonates given for cancer that has spread to the bone.
- Avascular necrosis caused by long-term use of corticosteroids.
- Pain syndromes caused by radiation therapy, including:
- Pain from brachytherapy.
- Pain from lying in the same position during treatment.
- Mucositis (inflammation of the mucous membranes in areas that were treated with radiation).
- Dermatitis (inflammation of the skin in areas that were treated with radiation).
- Pain flares (a sudden increase of pain in the treated area).
Peripheral neuropathy is a type of pain that can be caused by chemotherapy.
Peripheral neuropathy is a nerve problem that can cause pain, numbness, and tingling in the hands and feet. Patients on chemotherapy may have chemotherapy-induced peripheral neuropathy (CIPN). In some patients, CIPN may continue after chemotherapy has ended.
Studies of drugs and natural products used to treat CIPN have shown mixed results. Duloxetine is a drug that has been studied to treat CIPN.
Studies of acupuncture for CIPN have been reported. See the Chemotherapy-induced peripheral neuropathy section in the PDQ summary on Acupuncture for information about these studies.
Cancer pain may affect quality of life and ability to function even after treatment ends.
Pain that is severe or continues after cancer treatment ends increases the risk of anxiety and depression. Feeling depressed or having anxiety can worsen cancer pain and make it harder to control. Some patients are unable to work because of the pain.
Pain control can improve your quality of life.
Pain can be controlled in most patients who have cancer. Although cancer pain cannot always be relieved completely, there are ways to lessen pain in most patients. Pain control can improve your quality of life during cancer treatment and after it ends.
Each patient needs a personal plan to control cancer pain.
Each person’s diagnosis, cancer stage, response to pain, and personal likes and dislikes are different. For this reason, each patient needs a personal plan to control cancer pain. You, your family, and your healthcare team can work together to manage your pain. As part of your pain control plan, your healthcare provider can give you and your family members written instructions to manage your pain at home. Ask your healthcare provider who you should call if you have questions about your pain.
Assessment of Cancer Pain
KEY POINTS
- Your healthcare team will ask you about your pain to determine the best treatment.
- Physical and neurological exams will be done to help plan pain control.
Your healthcare team will ask you about your pain to determine the best treatment.
It’s important that the cause of your pain is found early and treated quickly. Your healthcare team will help you measure pain levels often, including at the following times:
- After starting cancer treatment.
- After starting any type of pain treatment.
- When there is new pain.
To learn about your pain, the healthcare team will ask you the following questions:
- When did the pain start?
- How long does the pain last?
- Where is the pain? You will be asked to show exactly where the pain is on your body or on a drawing of a body.
- How strong is the pain? You will be asked to rate your pain between 1-10, with 10 being the strongest.
- Have there been changes in where or when the pain occurs?
- What makes the pain better or worse?
- Is the pain worse during certain times of the day or night?
- Is there breakthrough pain (intense pain that flares up quickly even when pain control medicine is being used)?
- Do you have trouble sleeping, or do you feel tired, depressed, or anxious?
- Does pain get in the way of activities of daily life, such as eating, bathing, or moving around?
Your healthcare team will also review your health history, including the following information:
- Past and current pain treatments.
- Prognosis (chance of recovery).
- Other conditions you may have, such as kidney, liver, or heart disease.
- Past and current use of nicotine, alcohol, or sleeping pills.
- Personal or family history of substance use disorder.
- Personal history of mental health disorders or abuse.
- Your choices for your pain control plan.
The information you give your healthcare team will be used to decide how to help relieve your pain. Treatment may include drugs or non-drug therapies. In some cases, patients are referred to pain or palliative care specialists. Your healthcare team will work with you to decide whether the benefits of treatment outweigh any risks. They will also let you know how much relief to expect from your pain treatment. After pain control is started, the doctor will continue to ask you how well your treatment is working and make changes if needed.
A family member or caregiver may be asked to give answers for a patient who has problems with speech, language, or understanding.
Physical and neurological exams will be done to help plan pain control.
The following exams will be done:
- Physical exam: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual.
- Neurological exam: A series of questions and tests to check the brain, spinal cord, and nerve function. The exam checks your mental status, coordination, and ability to walk normally, and how well the muscles, senses, and reflexes work. This may also be called a neuro exam or a neurologic exam.
Your healthcare team will also assess your psychological, social, and spiritual needs.
Using Drugs to Control Cancer Pain
KEY POINTS
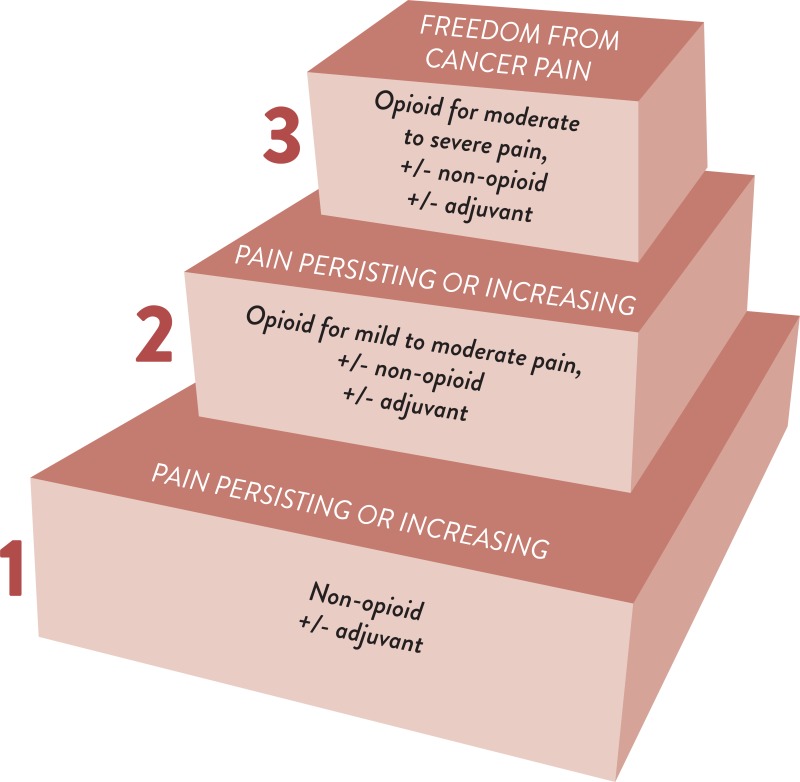
- The doctor will prescribe drugs based on whether the pain is mild, moderate, or severe.
- Acetaminophen and nonsteroidal anti-inflammatory drugs (NSAIDs) may be used to relieve mild pain.
- Opioids are used to relieve moderate to severe pain.
- Most patients with cancer pain will receive opioids on a regular schedule.
- Opioids are given in different ways.
- There are common side effects caused by opioids.
- Other drugs may be added to help treat your pain.
The doctor will prescribe drugs based on whether the pain is mild, moderate, or severe.
Your doctor will prescribe drugs to help relieve your pain. These drugs need to be taken at scheduled times to keep a constant level of the drug in the body to help keep the pain from coming back. Drugs may be taken by mouth or given in other ways, such as by infusion or injection.
Your doctor may prescribe extra doses of a drug that can be taken as needed for pain that occurs between scheduled doses of the drug. The doctor will adjust the drug dose for your needs.
A scale from 0 to 10 is used to measure how severe the pain is and decide which pain medicine to use. On this scale:
- 0 means no pain.
- 1 to 3 means mild pain.
- 4 to 6 means moderate pain.
- 7 to 10 means severe pain.
Other pain scales that use happy or sad faces may be used for those who have trouble giving their pain a number. These scales are also useful for adults who have trouble with memory or thinking, and with young children.
Acetaminophen and nonsteroidal anti-inflammatory drugs (NSAIDs) may be used to relieve mild pain.
Acetaminophen and NSAIDs help relieve mild pain. They may be given with opioids for moderate to severe pain.
Pain relievers of this type include:
Side effects of NSAIDs include stomach, kidney, heart, and blood problems. Patients, especially older patients, who are taking acetaminophen or NSAIDs need to be closely watched for side effects. See Treating Cancer Pain in Older Patients for more information.
Opioids are used to relieve moderate to severe pain.
Opioids work very well to relieve moderate to severe pain. Some patients with cancer stop getting pain relief from opioids if they take them for a long time. This is called tolerance. Larger doses or a different opioid may be needed if your body stops responding to the same dose. Tolerance of an opioid is a physical dependence on it. This is not the same as addiction (psychological dependence).
Since 1999, the number of prescriptions written for opioids and the number of deaths caused by drug overdose in the United States have increased. Although most patients who are prescribed opioids for cancer pain use them safely, some patients may become addicted to opioids. Your doctor will carefully prescribe and monitor your opioid doses so that you are treated for pain safely.
There are several types of opioids:
- Buprenorphine.
- Codeine.
- Diamorphine.
- Fentanyl.
- Hydrocodone.
- Hydromorphone.
- Methadone.
- Morphine (the most commonly used opioid for cancer pain).
- Oxycodone.
- Oxymorphone.
- Tapentadol.
- Tramadol.
The doctor will prescribe drugs and the times they should be taken in order to best control your pain. Also, it is important that patients and family caregivers know how to safely use, store, and dispose of opioids.
Most patients with cancer pain will receive opioids on a regular schedule.
Receiving opioids on a regular schedule helps relieve the pain and keeps it from getting worse. The amount of time between doses depends on which opioid you are taking. The best dose is the amount of opioid that controls your pain with the fewest side effects. If opioid tolerance does occur (the opioid no longer works at the dose you are given), the dose may need to be increased or a different opioid may be prescribed.
Opioids are given in different ways.
Opioids may be given by the following ways:
- Mouth: If your stomach and intestines work normally, medicine is usually given by mouth. Opioids given orally are easy to use and are usually low-cost. Oral opioids are sometimes placed under the tongue (sublingual route) or on the inside of the cheek (buccal route) to be absorbed.
- Rectum: If you cannot take opioids by mouth, they may be given as rectal suppositories.
- Skin patches: Opioid patches are placed on the skin (transdermal route).
- Nose spray: Opioids may be given in the form of a nasal spray.
- Intravenous (IV) line: Opioids are given into a vein only when simpler and less costly methods cannot be used, don’t work, or are not wanted by the patient. Patient-controlled analgesia (PCA) pumps are one way to control pain through your IV line. A PCA pump allows you to control the amount of drug that is used. With a PCA pump, you can receive a preset opioid dose by pressing a button on a computerized pump that is connected to a small tube. Once the pain is controlled, the doctor may prescribe regular opioid doses based on the amount you used with the PCA pump.
- Subcutaneous injection: Opioids are given by injection into the fatty layer of tissue just under the skin.
- Intraspinal injection: Intraspinal opioids are injected into the fluid around the spinal cord. These may be combined with a local anesthetic to help some patients who have pain that is hard to control.
There are common side effects caused by opioids.
Your doctor will discuss the side effects with you before opioid treatment begins and will watch you for side effects. The following are the most common side effects:
- Nausea.
- Drowsiness.
- Constipation.
Nausea and drowsiness most often occur when opioid treatment is first started and usually get better within a few days.
Opioids slow down the muscle contractions and movement in the stomach and intestines, which can cause hard stools. To keep the stool soft and prevent constipation, it’s important to drink plenty of fluids, increase fiber in the diet, and get regular exercise, in addition to taking laxatives. Unless there are problems such as a blocked bowel or diarrhea, you will be given a treatment plan to prevent constipation and other digestive problems while taking opioids.
Other side effects of opioid treatment include the following:
- Dry mouth.
- Vomiting.
- Low blood pressure.
- Dizziness.
- Trouble sleeping.
- Trouble thinking clearly.
- Delirium or hallucinations.
- Trouble urinating.
- Problems with breathing, which may be worsened by sleep apnea, obesity, or combining opioids with sedatives.
- Severe itching.
- Problems with sexual function.
- Hot flashes.
- Depression.
- Hypoglycemia.
Talk to your doctor about side effects that bother you or become severe. Your doctor may decrease the dose of the opioid, change to a different opioid, or change the way the opioid is given to help decrease the side effects. See the following PDQ summaries for more information about coping with these side effects:
- Gastrointestinal Complications
- Nausea and Vomiting Related to Cancer Treatment
- Delirium
Other drugs may be added to help treat your pain.
Other drugs may be given while you are taking opioids for pain relief. These are drugs that help the opioids work better, treat symptoms, and relieve certain types of pain. The following types of drugs may be used:
- Antidepressants.
- Anticonvulsants.
- Local anesthetics.
- Corticosteroids.
- Bisphosphonates and denosumab.
There are big differences in how patients respond to these drugs. Side effects are common and should be reported to your doctor.
Bisphosphonates (pamidronate, zoledronic acid, and ibandronate) are drugs that are sometimes used when cancer has spread to the bones. They are given as an intravenous infusion and combined with other treatments to decrease pain and reduce risk of broken bones. However, bisphosphonates sometimes cause severe side effects. Talk to your doctor if you have severe muscle or bone pain. Bisphosphonate therapy may need to be stopped.
The use of bisphosphonates is also linked to the risk of bisphosphonate-associated osteonecrosis (BON). See the PDQ summary on Oral Complications of Chemotherapy and Head/Neck Radiation for more information.
Denosumab is another drug that may be used when cancer has spread to the bones. It is given as a subcutaneous injection and may help prevent and relieve pain.
Other Treatments for Cancer Pain
KEY POINTS
- Nerve blocks
- Neurological treatments
- Cordotomy
- Palliative care
- Radiation therapy
- External radiation therapy
- Radiopharmaceuticals
- Physical medicine and rehabilitation
- Integrative therapies
Most cancer pain can be controlled with drugs, but some patients have too many side effects from drugs or have pain in a certain part of the body that needs to be treated in a different way. Talk to your doctor to help decide which methods work best to relieve your pain. Other treatments include:
Nerve blocks
A nerve block is the injection of either a local anesthetic or other drug into or around a nerve to block pain. Nerve blocks help control pain that can’t be controlled in other ways. Nerve blocks may also be used to find where the pain is coming from, to predict how the pain will respond to long-term treatments, and to prevent pain after certain procedures.
Neurological treatments
Surgery can be done to insert a device that delivers drugs or stimulates the nerves with mild electric current.
Cordotomy
Cordotomy is a less common surgical procedure that is used to relieve pain by cutting certain nerves in the spinal cord. This blocks pain and hot/cold feelings. This procedure may be chosen for patients who are near the end of life and have severe pain that cannot be relieved in other ways.
Palliative care
Certain patients are helped by palliative care services. Palliative care providers may also be called supportive care providers. They work in teams that include doctors, nurses, mental health specialists, social workers, chaplains, pharmacists, and dietitians. Some of the goals of palliative care are to:
- Improve quality of life for patients and their families.
- Manage pain and non-pain symptoms.
- Support patients who need higher doses of opioids, have a history of substance use disorder, or are coping with emotional and social problems.
See the PDQ summary on Planning the Transition to End-of-Life Care in Advanced Cancer for more information.
Radiation therapy
Radiation therapy is used to relieve pain in patients with skin lesions, tumors, or cancer that has spread to the bone. This is called palliative radiation therapy. It may be given as local therapy directly to the tumor or to larger areas of the body. Radiation therapy helps drugs and other treatments work better by shrinking tumors that are causing pain. Radiation therapy may help patients with bone pain move more freely and with less pain.
The following types of radiation therapy may be used:
External radiation therapy
External radiation therapy uses a machine outside the body to send high-energy x-rays or other types of radiation toward the area with cancer. External radiation therapy relieves pain from cancer that has spread to the bone. Radiation therapy may be given in a single dose or divided into several smaller doses given over time. The decision to have a single or divided dose may depend on how easy it is to get the treatments and how much they cost. Some patients who find little or no pain relief from first-time radiation therapy may benefit from repeated radiation therapy.
Patients may have a pain flare (a temporary worsening of pain in the treated area) after receiving palliative radiation therapy for cancer that has spread to the bone, but this side effect is only temporary.
Radiopharmaceuticals
Radiopharmaceuticals are drugs that have a radioactive substance that may be used to diagnose or treat disease, including cancer. Radiopharmaceuticals may also be used to relieve pain from cancer that has spread to the bone. A single dose of a radioactive agent injected into a vein may relieve pain when cancer has spread to several areas of bone and/or when there are too many areas to treat with external radiation therapy.
Physical medicine and rehabilitation
Patients with cancer and pain may lose their strength, freedom of movement, and ability to manage their daily activities. Physical therapy or occupational therapy may help these patients.
Physical medicine uses physical methods, such as exercise and machines, to prevent and treat disease or injury.
Some patients may be referred to a physiatrist (a doctor who specializes in physical medicine) who can develop a personal plan for them. Some physiatrists are also trained in procedures to treat and manage pain.
Integrative therapies
Complementary and alternative therapies combined with standard treatment may be used to treat pain. They may also be called integrative therapies. Acupuncture, support groups, and hypnosis are a few integrative therapies that have been used to relieve pain.
Treating Cancer Pain in Older Patients
KEY POINTS
- Certain factors affect cancer pain treatment in older adults.
- Older patients may be prescribed more than one drug.
- Doses start at lower levels.
- Side effects from drugs are more likely in older patients.
- There is a risk of undertreatment (not receiving enough treatment) in older patients.
Certain factors affect cancer pain treatment in older adults.
Some problems are more likely in patients 65 years and older. For caregivers of these patients, the following should be kept in mind:
Older patients may be prescribed more than one drug.
Older patients may have more than one chronic disease and take several drugs for different conditions. This can increase the risk of drug interactions. Drugs taken together can change how they work in the body and can affect the patient’s chronic diseases.
Doses start at lower levels.
Pain medicine is started at lower doses in older patients and adjusted slowly to allow for differences in their pain threshold, pain expression, and effects on physical and mental function. Lower doses given to older patients may provide better pain relief that lasts longer than in younger patients.
Side effects from drugs are more likely in older patients.
Older patients should be watched closely for side effects from opioids and NSAIDs. See common side effects caused by opioids for more information. Other drugs may be given to avoid side effects from certain NSAIDs:
- Acetaminophen.
- Proton pump inhibitors (given with NSAIDs).
- Topical NSAIDs.
- COX-2-selective NSAIDs (NSAIDs that cause fewer problems with the stomach and intestines).
There is a risk of undertreatment (not receiving enough treatment) in older patients.
Undertreatment in older patients may occur for the following reasons:
- Patients do not report their pain.
- Patients are not able to talk about the pain they have.
- The doctor is concerned about side effects or changes in patient behavior that may be caused by pain medicine.
Poor pain control may cause other problems in older patients, including the following:
- Reduced physical or mental function.
- Slow recovery.
- Changes in appetite or sleep.
- Increased need for care and assistance with health problems.
Treating depression in patients can also help with pain treatment.
The Opioid Epidemic and Cancer Pain Management: A Conversation with Dr. Judith Paice