A cluster headache is an uncommon type of headache. It is one-sided head pain that may involve tearing of the eyes, a droopy eyelid, and a stuffy nose. Attacks last from 15 minutes to 3 hours, occur daily or almost daily for weeks or months.
The attacks are separated by pain-free periods that last at least 1 month or longer.
Cluster headaches may be confused with other common types of headaches such as migraines, sinus headache, and tension headache.
What is cluster headache?
Cluster headache is a condition considered to be one of the worst pains known to man.
It affects up to 4 in 1000 people, similar to the incidence of multiple sclerosis and Parkinson’s disease.
It affects more men than women, making it unusual among headache disorders.
A family history of cluster headache is rare (only 3–5% of cases are hereditary).
The word ‘cluster’ refers to a period of time (weeks or months) during which the individual suffers recurrent attacks (cluster periods or bouts); the start of bouts often coincides with season changes, and with the times of year with the most or fewest hours of daylight.
Cluster headache presents in two distinct clinical forms: episodic and chronic. The most common is the episodic form which affects 80 to 90% of patients. In episodic cluster headache, subjects have cluster periods, or bouts, during which they experience one to eight attacks per day (with or without pain-free days) and periods of remission lasting more than 30 days. The typical patient has one bout per year, often at the same time of year. The chronic form is diagnosed after one year of pain without remission, or in subjects with remission periods of less than one month.
Attacks consist of a severe stabbing pain rapidly peaking at an unbearable intensity, usually lasting between 15 and 180 minutes, affecting one side (and nearly always the same side) of the head, and usually located in and around the orbit and in the temporal area. The pain is often likened to a ‘hot poker’ penetrating one eye.
During bouts, attacks recur at typical times, such as the middle of the night and around 3 and 9 p.m.
Out of a number of symptoms at least one will also occur during an attack:
Eyes may become red and watery.
Nasal congestion.
Running from the nostril.
Forehead and facial sweating.
Constriction of the pupil.
Drooping or swelling of the eyelid.
Physical agitation and tendency to move around.
The exact cause of cluster headache is unknown, but recent findings favor a dysfunction of the pain network.
Causes of Cluster Headache
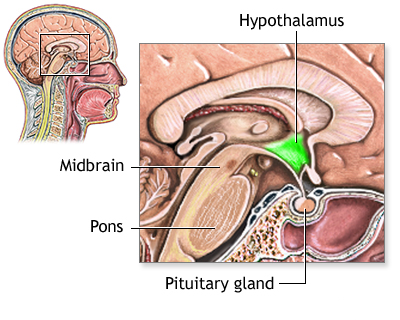
Doctors do not know exactly what causes cluster headaches. They seem to be related to the body’s sudden release of histamine (chemical in the body released during an allergic response) or serotonin (chemical made by nerve cells) in the area of a nerve in the face called the trigeminal nerve. A problem in a small area at the base of the brain called the hypothalamus may be involved.
More men than women are affected. The headaches can occur at any age, but are most common in the 20s through middle age. They tend to run in families.
Cluster headaches may be triggered by:
Symptoms of Cluster Headache
A cluster headache begins as a severe, sudden headache. The headache commonly strikes 2 to 3 hours after you fall asleep. But it can also occur when you are awake. The headache tends to happen daily at the same time of day. Attacks can last for months. They can alternate with periods without headaches (episodic) or they can go on for a year or more without stopping (chronic).
Cluster headache pain is usually:
- Burning, sharp, stabbing, or steady
- Felt on one side of the face from neck to temple, often involving the eye
- At its worst within 5 to 10 minutes, with the strongest pain lasting 30 minutes to 2 hours
When the eye and nose on the same side as the head pain are affected, symptoms can include:
- Swelling under or around the eye (may affect both eyes)
- Excessive tearing
- Red eye
- Droopy eyelid
- Runny nose or stuffy nose on the same side as the head pain
- Red, flushed face, with extreme sweating
Exams and Tests of Cluster Headache
Your health care provider can diagnose this type of headache by performing a physical exam and asking about your symptoms and medical history.
If a physical exam is done during an attack, the exam will usually reveal Horner syndrome (one-sided eyelid drooping or a small pupil). These symptoms will not be present at other times. No other nervous system (neurologic) changes will be seen.
Tests, such as an MRI of the head, may be needed to rule out other causes of the headaches.
Treatment of Cluster Headache
While there is currently no cure for cluster headache, the available treatment has become much more effective in the last 20 years.
Acute treatment is used to stop the pain once it has started. Treating cluster headache can be tricky because the pain becomes extremely severe very quickly – usually within a few minutes. Thus the key to treating a cluster headache attack is speed, to reduce the excruciating pain as fast as possible.
Ordinary painkillers that you can buy over the counter are not usually effective, as the pain of cluster headache is too intense and they take too long to work. Opioids are not effective either.
Oxygen is one of the safest ways to treat cluster headache. You need to breathe the oxygen in at a rate of between 10 and 15 liters per minute using a non-rebreathing mask, i.e. one without holes, for 15 minutes at the start of the attacks. The treatment usually starts to work within 10 to 15 minutes.
Your provider may recommend the following treatments for when the headaches occur:
- Triptan medicines, such as sumatriptan (Imitrex).
- Anti-inflammatory (steroid) medicines such as prednisone. Starting with a high dose, then slowly decreasing it over 2 to 3 weeks.
- Breathing in 100% (pure) oxygen.
- Injections of dihydroergotamine (DHE), which can stop cluster attacks within 5 minutes (Warning: this drug can be dangerous if taken with sumatriptan).
- Fioricet
You may need more than one of these treatments to control your headache. Your provider may have you try several medicines before deciding which works best for you.
Pain medicines and narcotics do not usually relieve cluster headache pain because they take too long to work.
Surgical treatment may be recommended for you when all other treatments have failed. One such treatment is a neurostimulator. This device delivers tiny electrical signals to certain nerves such as the occipital nerve in the scalp. Your provider can tell you more about surgery.
Prevention of Cluster Headache
Avoid smoking, alcohol use, certain foods, and other things that trigger your headaches. A headache diary can help you identify your headache triggers. When you get a headache, write down the following:
- Day and time the pain began
- What you ate and drank over the past 24 hours
- How much you slept
- What you were doing and where you were right before the pain started
- How long the headache lasted and what made it stop
Review your diary with your provider to identify triggers or a pattern to your headaches. This can help you and your provider create a treatment plan. Knowing your triggers can help you avoid them.
The headaches may go away on their own or you may need treatment to prevent them. The following medicines may also be used to treat or prevent headache symptoms:
- Allergy medicines
- Antidepressants
- Blood pressure medicines
- Seizure medicine
Preventative treatment is used throughout the entire course of the cluster period in an attempt to reduce the frequency and severity of cluster attacks. A wide range of preventative treatments is available and research on the effectiveness of possible new targeted prophylactic medications is ongoing.
The most common currently used preventative treatments are:
Verapamil: verapamil may be prescribed for cluster headache as research has shown that a daily dose can be effective in both episodic and chronic cluster headache.
As verapamil can disturb heart rhythms, patients may need ECG testing whilst the correct dose is being established. Any patients with an underlying condition will require careful ongoing monitoring should they require high doses of verapamil.
Corticosteroids, as tablets or local injections: these are given because they are fast acting. They can be used in a short burst, for 2 to 3 weeks, in decreasing amounts as a first step to break the cycle. They are often used alongside other treatments, which take longer to work. They can only be recommended as transitory treatments in short cycles, as long-term treatments are associated with significant side effects.
Other options that can be considered are lithium carbonate, topiramate, valproic acid, gabapentin and baclofen.
As with any drug treatment you may need to work with your doctor to determine what works best for you. You may need to try several treatment regimens before you discover the best one for you and a referral to a headache specialist can be recommended.
When to Contact a Medical Professional
Call 911 if:
- You are experiencing “the worst headache of your life.”
- You have speech, vision, or movement problems or loss of balance, especially if you have not had these symptoms with a headache before.
- A headache starts suddenly.
Schedule an appointment or call your provider if:
- Your headache pattern or pain changes.
- Treatments that once worked no longer help.
- You have side effects from your medicine.
- You are pregnant or could become pregnant. Some medicines should not be taken during pregnancy.
- You need to take pain medicines more than 3 days a week.
- Your headaches are more severe when lying down.
Prevention of Cluster Headache
If you smoke, now is a good time to stop. Alcohol use and any foods that trigger a cluster headache may need to be avoided. Medicines may prevent cluster headaches in some cases.
Alternative Names
Histamine headache; Headache – histamine; Migrainous neuralgia; Headache – cluster; Horton’s headache; Vascular headache – cluster; Episodic cluster headache; Chronic cluster headache
What is the Difference Between Migraine and Cluster Headache?
One of the main differences between migraine and cluster headache is that the person with cluster headache, unlike the person with migraine, becomes agitated during an attack and is unable to sit or lie down or find relief in sleeping. Where a migraine can last up to 72 hours, a cluster headache lasts less than 3 hours with the intensity of the pain peaking within a few minutes and reducing quickly at the end of the attack.
Commandments for Health Professionals
Cluster headache patients have issued the following 7 Commandments to Health Professionals for better treatment of those who live with cluster headache:
Ensure early and accurate diagnosis and treatment.
Know and educate colleagues about the clinical signs of cluster.
Provide accurate and reliable information and dispel the myths.
Listen to the person, acknowledge the condition, and reassure them as you provide the care.
Recognize the impact and burden on all those affected, both at home and at work.
Encourage the person to speak about their disorder in all aspects of their life and engage with their patient community.
Ensure easy access to headache specialists and provide ongoing support.
If you have met a doctor who observes these Commandments you are in good hands … You can recommend him/her to others with the same problem.